
Abstract

Imaging Clinic
A 61-year-old male was referred to the ear, nose, and throat clinic after presenting to the emergency department with epistaxis and a gradually enlarging oral mass. He denied any hoarseness, dysphasia, or associated pain. He has significant history of smoking and alcohol use. Otherwise, he has no known medical problems or prior surgery.
Panendoscopy was performed and revealed a large exophytic lesion emanating from the left posterior maxilla involving the left vestibule of the mouth. Biopsy with histopathologic analysis revealed renal cell carcinoma (RCC) of clear cell type (Figure 1 A-F). Computed tomography (CT) of the head and neck demonstrated involvement of left maxillary sinus with bony destruction and mucosal thickening in the adjacent portion of the maxillary sinus (Figure 2). Given the histologic findings, a CT of the abdomen was obtained and showed a left renal mass (Figure 3) with imaging characteristics compatible with RCC. The patient is subsequently undergoing treatment with radiation therapy.
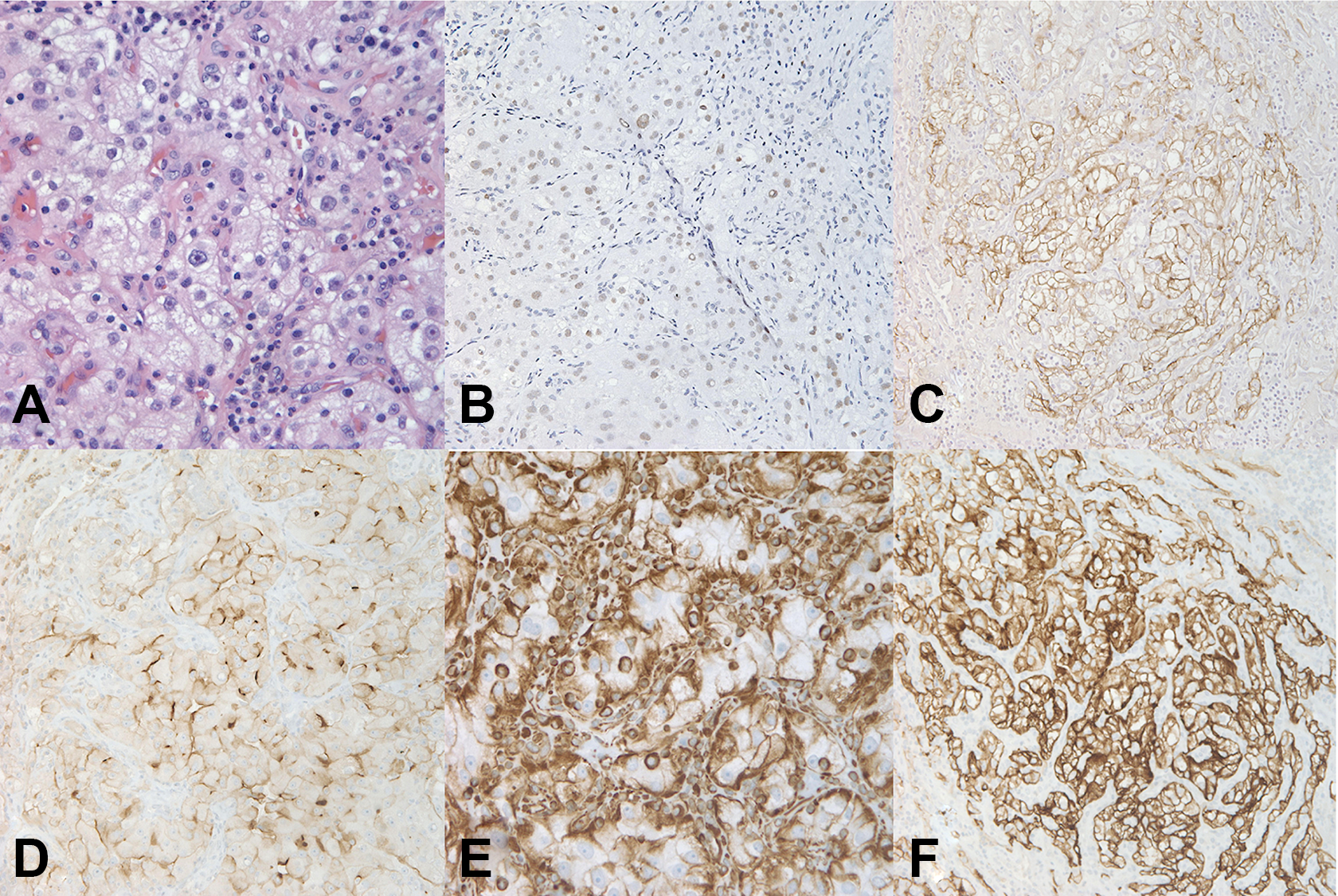
A to F, Histopathological stain. Within the submucosa, there is an infiltration of nested clear tumor cells interspersed by a prominent capillary network. The nuclei are moderately pleomorphic with irregular contours and have prominent nucleoli, indicative of a high nuclear grade (A). Tumor cells are positive for paired box gene 8 (PAX8) [B], cytokeratin AE1/AE3 (C), CD10 (D), vimentin (E), and CAM 5.2 (F). Stains for thyroid transcription factor [TTF-1], S100, and desmin are negative. The morphology and immunoprofile of the lesion are highly suggestive of a metastatic renal cell carcinoma.
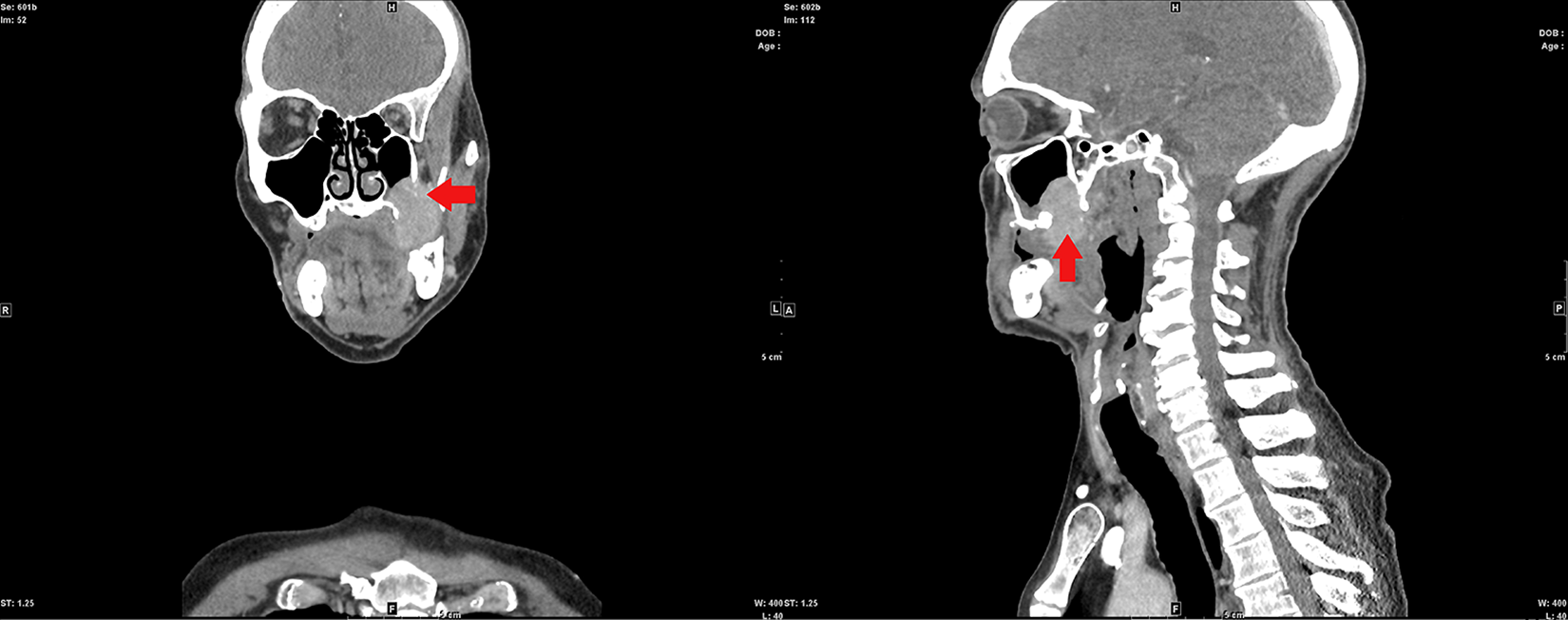
Contrast CT of the head and neck. Coronal and sagittal image showed a well-marginated, heterogeneous, enhancing mass measuring 3.4 × 2.2 × 2.2 cm. It appears to be originating in the left posterior inferolateral maxillary wall with bony destruction and extension into the masticator space, posterior portion of the superior alveolar ridge, and retromandibular trigone. Also noted is mucosal thickening in the adjacent portion of the maxillary sinus. CT indicates computed tomography.
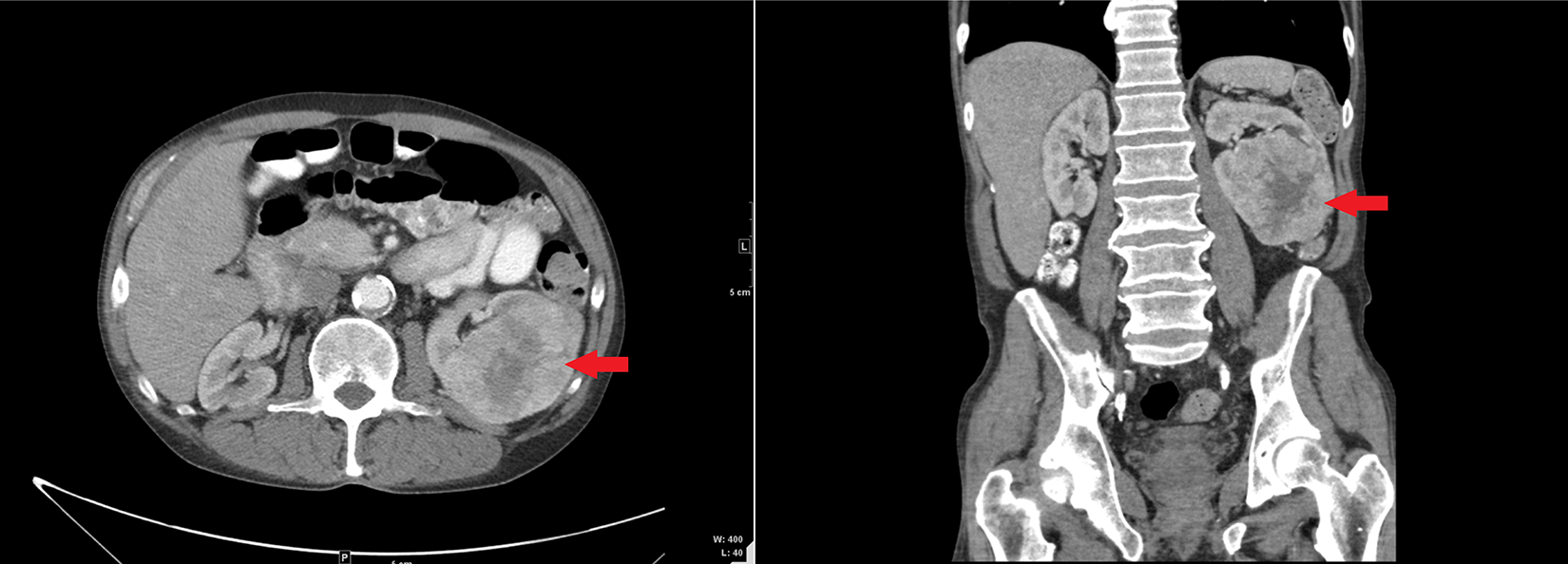
Computed tomography (CT) with contrast of the abdomen. Axial and coronal image of the abdomen showing an 8.7 × 8.1 × 7.2 cm heterogeneously enhancing mass involving the mid and inferior aspect of the left kidney.
Renal cell carcinoma presents as a solid, lobulated, well-circumscribed, yellow mass that may have necrosis or red discoloration due to hemorrhage on gross examination. Renal cell carcinoma typically present in patients over the age of 40 with a male preponderance. 1 Clear cell renal cell carcinoma accounts for 70% of renal epithelial tumors. Microscopically, hematoxylin-eosin staining shows optically clear cytoplasm due to glycogen and lipid loss during processing, with a highly recognizable alveolar-like vascular pattern. Blood lakes or bloody glands can be visualized within a cluster of cells, representing vastly vascularized areas that have hemorrhaged. The cuboidal tumor cells have a centrally or basally located nucleus. 1
Metastasis occurs when malignant cells from the primary tumor deposit at distal sites via hematogenous or lymphatic supply. Renal cell carcinoma metastasis bypasses pulmonary capillary filtration due to its transportation along the inferior vena cava or Batson paravertebral venous plexus. 2 One in 3 patients will have metastasis from RCC within 3 years. The most common metastatic sites are lung, liver, bone, and rarely the head and neck. 1 When these rare metastatic events occur, RCC is the most common to metastasize to the paranasal region, specifically the maxillary sinus.
Biallelic inactivation of von Hippel-Lindau (VHL) tumor suppressor gene at 3p25.3 is implicated in RCC. 1 There is a loss of function of the VHL gene product (pVHL) caused by complete or partial loss, somatic mutation, or promotor hypermethylation. Hypoxia-inducible factor 1α (HIF-1α) is used by pVHL to regulate cell signaling by ubiquitin-mediated proteasomal degradation. 3 A loss of function in pVHL leads to HIF-1α accumulation. This accumulation results in an increased transcription of genes regulated by HIF, such as those involved in angiogenesis and cellular homeostasis.
The upregulation in genes makes it difficult to treat RCC with chemotherapy and radiotherapy, but a good target for drug therapy. The best treatment, however, relies on surgical excision of the tumor mass. Excision of the metastatic mass with a nephrectomy renders the patient with a 41% survival in 2 years and 13% in 5 years. Excising the metastatic mass alone lowers the survival rate. Having multiple metastatic masses significantly lowers the survival rate to 0% to 7% in 5 years. 4
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.