
Abstract
Objectives:
Children experience serious gastrointestinal tract injuries due to consumption of caustic agents more often than adults. The aim of the study was to analyze diagnostic methods and treatment of children with esophageal burns according to the degree of the injury.
Methods:
Our one-center population-based retrospective cohort study included 150 children admitted between 1967 and 2018 to Clinic of Pediatric Otolaryngology, Phoniatrics and Audiology of University Children’s Hospital in Lublin, Poland, due to the chemical burn of the mouth, throat, larynx, and esophagus. Each patient underwent a thorough laryngological examination and endoscopy to assess the place and degree of injury.
Results:
Of 150 patients, 65.3% were male and 34.7% female. The median age was 4 years and 3 months. Salivation, dysphagia, burning sensation, edema, and whitish coating on the oral mucosa, palate, and throat were the most common clinical symptoms. In addition, dyspnea and chest pain were observed in 30% of patients. Esophagus endoscopy results were: Zargar grade I burn (84.7%), grade IIA (8%), grade IIB (2.6%), grade III (0%), and grade 0 (4.7%). Treatment included antibiotics, proton pump inhibitors, analgesics, and intravenous fluid therapy. Late sequelae (scarred esophageal strictures) developed in 20 (13.3%) patients.
Conclusions:
Accidental intake of caustic agents is observed in young children, especially younger than the age of 5. Early esophagus endoscopy should be performed in all patients to assess the grade of injury, plan initial treatment, and predict the risk of developing complications. Early diagnosis and immediate pharmacological treatment reduce the number of late sequelae.
Introduction
Caustic substances are widespread and easily available in our everyday life. They differ in their activity and composition. The most common substance causing chemical burns of the digestive tract is sodium hydroxide.
Corrosive substances can be divided into acidic or alkaline. They can damage tissues in a variety of mechanisms. The acids lead to coagulation necrosis, resulting in a clot that prevents the agent penetration into the deeper tissues. 1 Alkali, however, leads to necrotic necrosis and saponification of fats and, due to hygroscopic properties, penetrates deeper into tissues. In addition, the bases cause thrombosis in the blood vessels, which limits blood flow within the damaged tissue. 2
It is estimated that 80% of the overall number of people injured due to ingestion of caustic agents are children, 3 which is explained by insufficient attention of careers. 4 In contrast, among adults, the vast majority are people deliberately consuming chemicals for suicide. The frequency of chemical burns caused by cleaning agents among children younger than 2 years is associated with their motor development and with the inappropriate storage of caustic substances in the household. 5
Severe corrosive poisoning can cause serious chemical damage to the upper gastrointestinal tract. The degree of the chemical burn depends on several factors, such as chemical properties of the substance, dose, concentration, duration of action, and individual properties of the body. The most common are burns of the mouth, throat, and esophagus. In developing countries, the number of cases of digestive tract burns with caustic substances is still growing, 6 which is related to social, economic, and educational factors, but most often results from the lack of appropriate prophylaxis. 7 The aim of our study was to analyze diagnostic methods and treatment of children with esophageal burns according to the degree of the injury.
Patients and Methods
Our one-center population-based retrospective cohort study included 150 children admitted between 1967 and 2018 to the Clinic of Pediatric Otolaryngology, Phoniatrics and Audiology of University Children’s Hospital in Lublin, Poland, due to the chemical burn of the mouth, throat, larynx, and esophagus. Signs and symptoms have been described immediately after otolaryngological examination. All children underwent early esophagus endoscopy to assess the site and extent of mucosal damage according to Zargar classification. 1 The Zargar classification consists of 4 grades: grade 0 means there is no damage and mucosa is normal. In grade I, edema and erythema are present. In grade IIA, we can find hemorrhage, erosions, blisters, and superficial ulcers, and in grade IIB, circumferential lesions are present. In grade IIIA, focal deep gray or brownish-black ulcers are found, and in IIIB, deep gray discoloration is more extensive. In grade IV, a perforation is present.
Ethical Approval/Clearance
The principles outlined in the Declaration of Helsinki were followed during the study. It was a retrospective study considering only the data in patients’ medical records.
Results
In our department, the ingestion of caustic agents was more frequent among males (65.3%) than females (34.7%). The age of children ranged from 5 months to 17 years, and the median age was 4 years and 3 months. Residents of cities constituted 54.7% of hospitalized patients, while 45.3% of patients lived in rural areas. The vast majority of children (80%) came from an environment with a low level of education and material status. None of the patients were diagnosed with any chronic disease. Salivation, dysphagia, burning sensation, edema, and whitish coating on the oral mucosa, palate, and throat were the most common clinical symptoms. In addition, dyspnea and chest pain were observed in 30% of patients. In each patient, flexible nasolaryngoscopy and esophagogastroduodenoscopy were performed. In 84.7% of patients, edema and mucosal hypersecretion were found, which correspond to Zargar grade I burn. Grade IIA burn was noted in 8% of participants, grade IIB only in 2.6%, grade III burns were not found, and in 4.7% of patients, the esophageal mucosa did not show signs of damage which corresponds to grade 0 of Zargar classification (Figure 1). The greatest mucosal injuries were observed in narrowest places, that is, at the level of physiological constrictions of the esophagus.
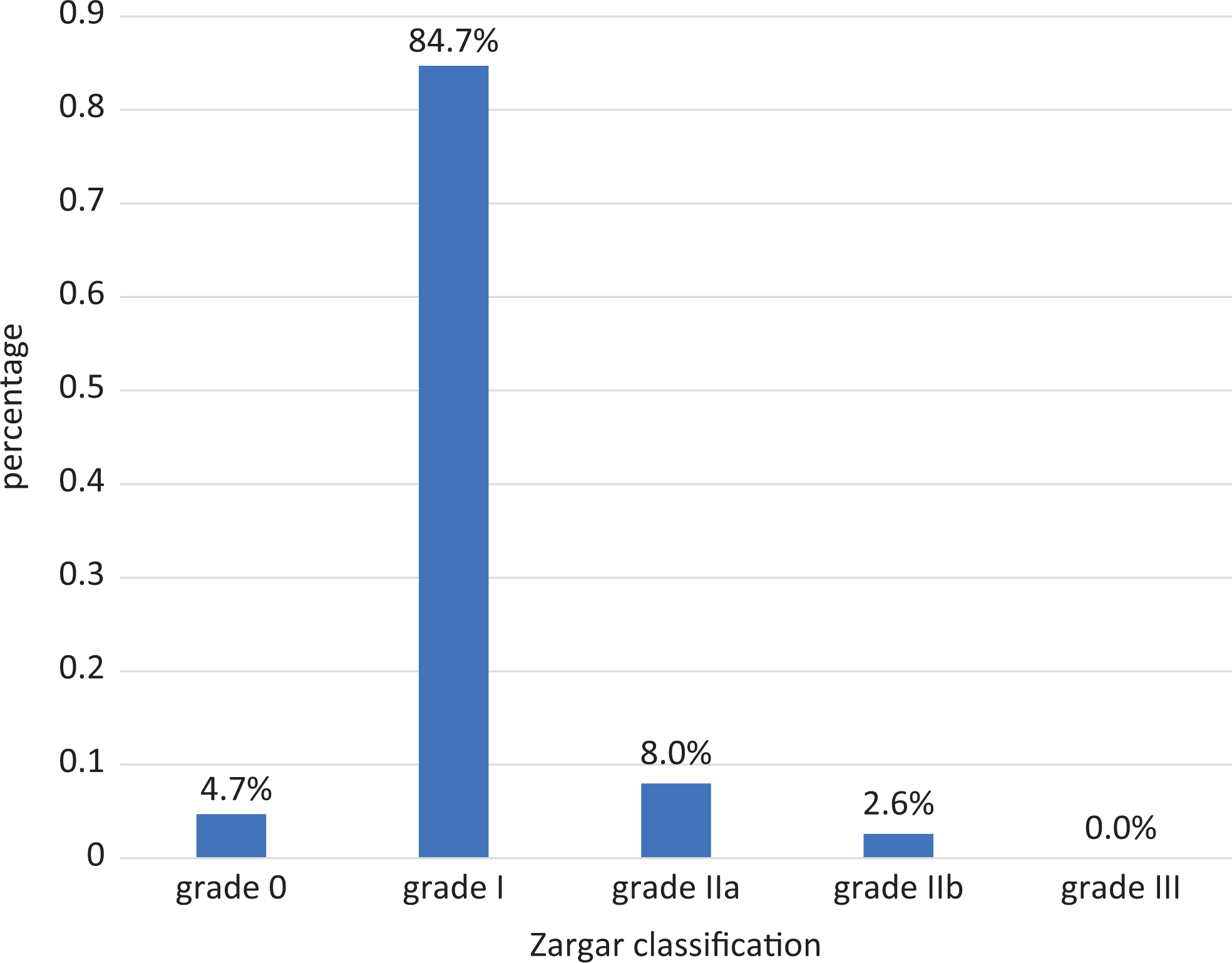
Grade of the esophagus burn injury according to the Zargar classification.
Gastrointestinal injuries were most often observed as a result of ingesting: cleaning products in 88 (58.7%) patients, hot water in 31 (20.3%) cases, hydrochloric acid in 10 (6.7%) patients, potassium permanganate in 10 (6.7%) patients, calcium hydroxide in 5 (3.3%) patients, and sodium hydroxide in 6 (4%; Figure 2). The most serious injuries were observed as a result of ingestion of calcium hydroxide and sodium hydroxide. Domestic bleaches are relatively nontoxic because they contain low sodium hypochlorite.
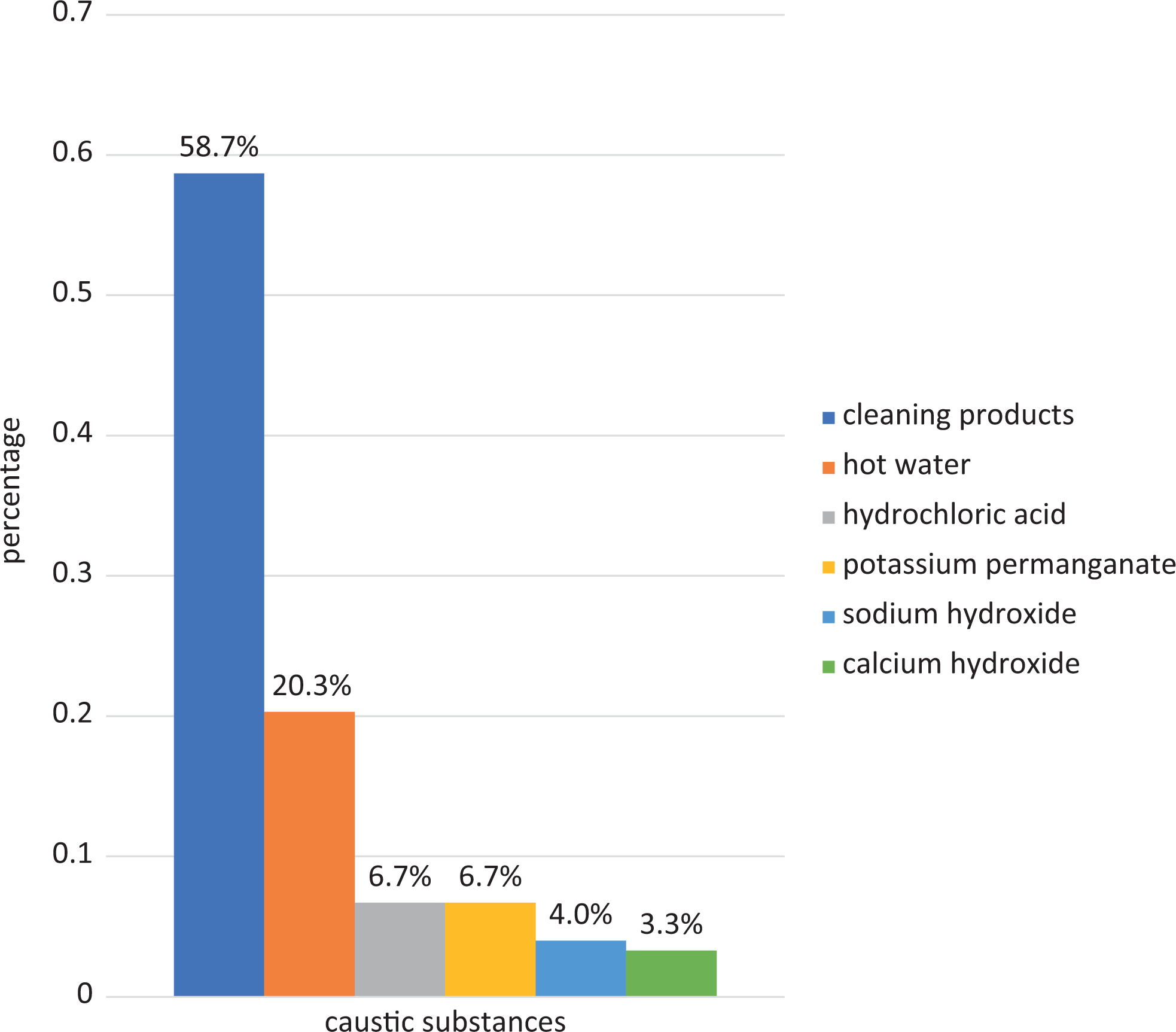
Types of caustic substance ingested by children.
The location of injuries depended on the chemical agent’s state of matter. In a group of 35 patients, ingestion of caustic agents in a solid state (in the form of a granular powder) resulted in injuries only in the mouth and throat, while the admission of liquid chemicals in 22 cases caused damage only within the esophagus.
The distribution of burns in case of drinking a scalding substance was different. Twenty-two (84.6%) of 26 cases of hot water consumption caused mucosal lesions in the mouth, throat, esophagus, and larynx, of which 16 of them were eroded and ulcerated. The gastric mucosa was damaged only in 2 (7.7%) patients, while the other 2 (7.7%) did not show any injuries.
All patients were treated with antibiotics, proton pump inhibitors, analgesics, and intravenous fluid therapy. Three (2%) children required tracheotomy as a result of inhalation of caustic substances into the lower respiratory tract. Late sequelae such as scarred esophageal strictures developed in 20 patients, which constituted 13.3% of the examined children. Endoscopic esophageal dilatation (EED) was successfully performed in 10 (6.7%) patients. In 2 (1.3%) cases intraesophageal incision and in 1 (0.6%) girl esophageal scar tissue removal were needed.
All patients were discharged home in good general condition with a recommendation for further control. We do not have sufficient data on all patients hospitalized for esophageal burn since 1967, so we cannot exclude the possible growth of malignant lesions in the area of scars.
Discussion
Accidental ingestion of corrosive compounds is observed in young children, especially those younger than the age of 5, 8 which is convergent with the results of our study, as the mean age of our patients was 4 years and 3 months.
In Barrón Balderas et al’s study, an esophageal burn was the most common consequence of caustic soda ingestion compared to other caustic agents. 9 In our study, cleaning products, which often contain caustic soda, resulted in most cases (58.7%) of esophageal injuries.
The clinical examination after the ingestion of a chemical substance focuses on the identification of the type of corrosive substance, its quantity, concentration, state of matter, time of exposure to tissues, the extent of the injury, and the risk assessment of the possible consequences. Choosing the appropriate therapy depends on all the abovementioned factors. The corrosive substance in the granulate or powder adheres to the mucous membrane of the mouth and throat causing the most serious injuries in situ, unlike fluids that are easily swallowed and may cause damage to further parts of the gastrointestinal tract, such as the esophagus and stomach. 10 Our research confirms these findings because in a group of 35 patients, ingestion of caustic agents in a solid state resulted in injuries only in the mouth and throat, while the admission of liquid chemicals in 22 cases caused damage only within the esophagus. Lack of changes in the mouth and throat does not exclude serious injury at the esophagus. 11 On the other hand, their presence is not a reliable indicator of damage to the esophagus. 12 Clinical symptoms that may occur after burns of the digestive tract include dyspnea, chest pain, dysphagia, odynophagia, salivation, abdominal pain, nausea, and vomiting. In our study, dyspnea and chest pain were observed in 30% of patients. Moreover, we found that the most common clinical symptoms included salivation, dysphagia, burning sensation, edema, and whitish coating on the oral mucosa, palate, and throat. Hoarseness, dysphonia, stridor, cough, or tachypnea may indicate damage to the airways. The relationship between symptoms and the degree of damage to the mucosa of the gastrointestinal tract is uncertain, 12 but several studies show that stridor and salivation are 100% specific for significant damage to the esophagus. 13
Flexible nasolaryngoscopy is used to assess the condition of both the larynx and throat. Endoscopy is the most effective and widely used method for determining the degree of injury and planning treatment. 14 It was performed in all of our patients.
Early esophageal endoscopy is considered a safe procedure during the first 24 to 48 hours. 15 All of our patients underwent the procedure. Contraindication to its implementation is radiological suspicion of perforation, as well as an epiglottis swelling suggesting burns of the airways, which is an urgent indication for intubation or tracheotomy. In our study, 3 (2%) children required tracheotomy as a result of inhalation of caustic substances into the lower respiratory tract. The control endoscopy of the esophagus should be carried out 3 weeks after the incident when the risk of perforation is the smallest. Although it is a mandatory procedure performed in patients who have clinical symptoms that indicate that the substance is corrosive, it is not necessary for asymptomatic patients, especially when the clinical interview is uncertain. 16
Conservative therapy conducted in all of our patients consisted of antibiotics, proton pump inhibitors, analgesics, and intravenous fluid therapy in our study. Cardiopulmonary stabilization, intravenous fluid therapy, and parenteral nutrition are crucial in the acute phase of the disease. Treatment of burns caused by swallowing corrosive substance also includes neutralization of chemical substance, antibiotic therapy, corticosteroid therapy, treatment with proton pump inhibitors, H2 receptor blockers, collagen synthesis inhibitors, and the use of more advanced medical activities, such as EED, stent implantation, and surgery. 17 Neutralization of toxic substances by buffer compounds is currently contraindicated. Some authors believe that the heat generated in the above chemical reaction may aggravate damage to the upper gastrointestinal tract. 18 The systemic administration of steroids is only recommended in cases of inflammatory edema of the upper respiratory tract, but it seems to be ineffective in preventing stenosis. 19 Sometimes, when the therapy does not give satisfactory results and the edema progresses, tracheotomy becomes necessary. On the other hand, focal steroid injections are used more and more often in parallel with an endoscopic esophageal widening in the case of refractory stenosis. 20 Furthermore, it has been documented that steroid injections are safe in pediatric patients. 21 The most common steroid used in the above therapy is triamcinolone acetate at a concentration of 40 mg/mL, 22 but the number of doses needed during therapy has not yet been established and requires standardization. 20 Omeprazole is a gastric H+/K+-ATPase (adenosine triphosphatase) inhibitor, which also has anti-inflammatory and antioxidant properties. 23 Proton pump inhibitors, such as H2 receptor antagonists, are widely used to treat chemical esophageal burns, but their efficacy has not yet been proven. However, several experimental studies have described the efficacy of omeprazole and vitamin E in the early and late phase of poisoning with caustic substances. 24 Çakal et al were the first to notice a significant improvement in both endoscopic and clinical imaging in patients after intravenous administration of omeprazole in the acute phase of intoxication. 25
Endoscopic esophageal dilatation can be started after the third week from poisoning. In our study, EED was performed in 10 (6.7%) patients. Dilatations can be made by balloon or bougies. If the procedure is performed in time, it has great importance in obtaining a good treatment effect. 26 Several clinical studies have shown that dilation of the esophagus performed too late, after ingestion of the corrosive substance, carries a higher risk of perforation and increases the frequency of recurrences. 7,27 Although endoscopic balloon dilatation (EBD) is generally considered to be a safe and effective procedure in children, 28 -33 the effectiveness of this procedure in patients with postoperative esophageal stenosis is low. 33 What’s more, the frequency of perforation after EBD is higher in the case of poisoning with caustic substances than in case of esophageal strictures formed in another mechanism. 34 Due to the significant percentage of failures after EBD, it should only be used for a limited number of children with postoperative esophageal stenosis. 35 In contrast to EBD, mechanical expansion (bougie) seems to be more useful in the case of heavy, long, scarred, and serious scars that arise as a result of poisoning with caustic substances. 36,37 In cases where dilatational methods are ineffective, stenting of the esophagus is performed. Promising effects were observed after using intraesophageal polytetrafluoroethylene and silicone stents. 38
Surgical treatment is becoming more popular due to the risk of malignant transformation at the site of narrowing, 39 such as squamous cell carcinoma. According to Arnold and Numanoglu, the risk of secondary esophageal carcinoma mandates long-term surveillance. 40 Unfortunately, our patients were lost to follow-up; however, a possible growth of malignant lesions in the area of scars cannot be excluded.
In conclusion, the consumption of caustic agents is a great threat to children’s lives, especially in developing countries. Despite the recommendations of storing poisonous substances in places inaccessible to children, beyond the reach of their eyes and hands, the incidence of accidental chemical poisonings mainly by cleaning products is still high. The methods of treatment and prognosis depend on the properties of the caustic substance, its physical state, amount, concentration, time of exposure to tissues, and extent of esophageal mucous membrane damage shown by endoscopic examination. Ingestion of caustic agents in a solid state usually results in injuries only in the mouth and throat, while the admission of liquid chemicals causes damage only within the esophagus. Most common clinical symptoms include salivation, dysphagia, burning sensation, edema, and whitish coating on the oral mucosa, palate, and throat. Early esophageal endoscopy should be performed in all patients to plan initial treatment and predict the risk of developing strictures. Early diagnosis and immediate pharmacological treatment with antibiotics, proton pump inhibitors, analgesics, and intravenous fluid therapy reduce the number of late sequelae. Endoscopic esophageal dilatation is still the most effective method of progressive narrowing treatment. Treatment of injuries caused by caustic agents is difficult and still remains a challenge for head and neck surgeons, children’s surgeons, and gastroenterologists.
Footnotes
Authors’ Note
All authors conceived the presented idea. All authors developed the theory and performed the computations. All authors verified the analytical methods. All authors discussed the results and contributed to the final manuscript. Correspondence and material requests should be addressed to corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.