
Abstract
Dermatomyositis is a rare multisystem autoimmune disorder occasionally accompanied by dysphagia. It is typically treated with immune modulating agents; however, dysphagia is often unresponsive to these. Previous reports have demonstrated the utility of videoflouroscopy and manometry in understanding the etiologies of dysphagia to inform a procedural target, historically the cricopharyngeus muscle. We present a case of dermatomyositis and dysphagia resistant to medical management in a patient found by videoflouroscopy and manometry to have severe oropharyngeal dysphagia, esophageal dysmotility and a cricopharyngeal web. We demonstrate the utility and safety of upper esophageal sphincter dilation by transnasal esophagoscopy even in the setting of multifactorial dysphagia.
A 29-year-old female with a complicated 9-year history of dermatomyositis presented to clinic with esophageal dysmotility and pharyngeal dysphagia recalcitrant to medical management, including intravenous immunoglobulin (IVIG). Years prior, she required placement of a jejunostomy tube for several episodes of aspiration pneumonia and continued to have inability to tolerate her secretions. A modified barium swallow (MBS) demonstrated difficulty with bolus traversion through the upper esophageal sphincter, as well as reduced pharyngeal squeeze (Figure 1). She then underwent a transnasal esophagoscopy and was found to have a thin cricopharyngeal web with an esophageal lumen less than 5 mm. She underwent successful balloon dilation to 15 mm. Following the dilation, she had symptomatic improvement, though it was marginal, and a repeat MBS with pharyngeal manometry was done to determine whether there was a role for further intervention (Figure 2).
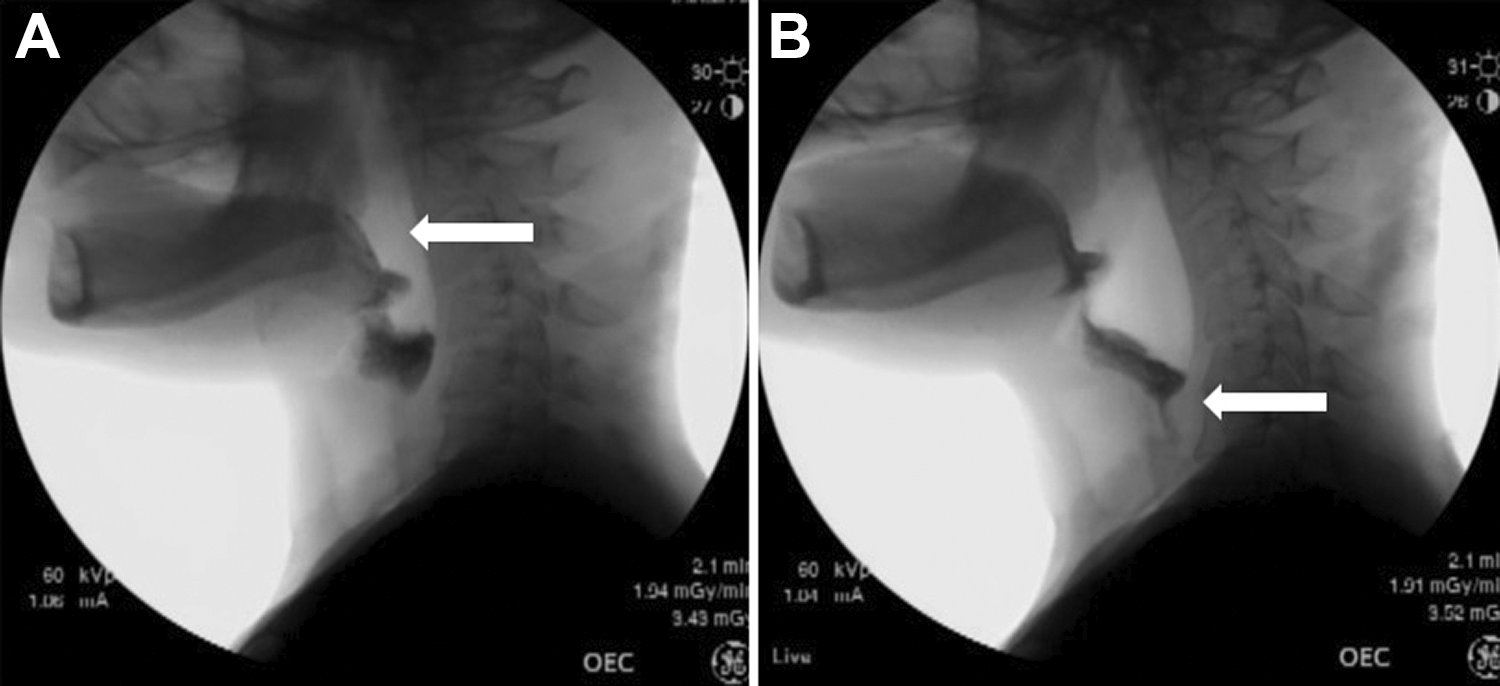
This is a series of videoflouroscopic images during a modified barium swallow study demonstrating lack of contact between base of tongue and posterior pharyngeal wall, with reduced pharyngeal squeeze (A) and narrowing at the upper esophageal sphincter (B).
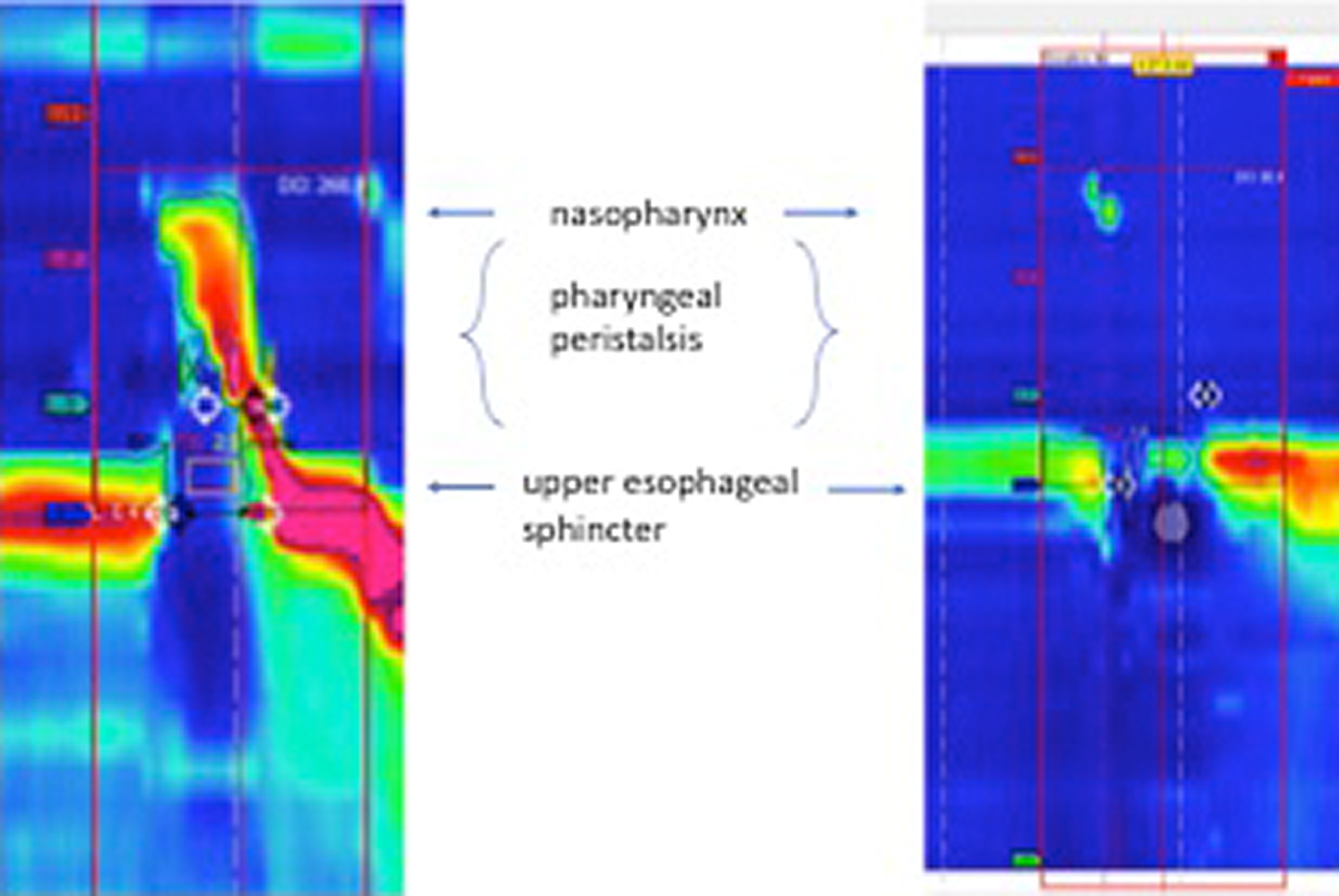
Normal pharyngeal manometry on the left with pharyngeal peristalsis, upper esophageal sphincter relaxation, and restoration of cricopharyngeal tone. On the right, the patient reveals absent pharyngeal peristalsis and a decreased upper esophageal sphincter or cricopharyngeus muscle tone.
Dermatomyositis is an idiopathic inflammatory myopathy that uncommonly presents with dysphagia. 1,2 Clinical characteristics include symmetric proximal muscle weakness, elevation of serum creatine phosphokinase, electromyographical demonstration of muscle impairment, abnormal muscle biopsy, and a skin rash. 1,2 Radiologic and videoflouroscopic findings of dysphagia may include pharyngeal pooling and a collapsed hypopharynx, impaired tongue base retraction or laryngeal elevation, hypertonic cricopharyngeal muscle, and poor or absent esophageal peristalsis. 2,3 Immunotherapeutic agents are the mainstay of treatment and include prednisone, methotrexate, mycophenalate, azathioprine, and IVIG. 3 Dysphagia is often steroid resistant and multifactorial, so procedural intervention should be directed at targets identified by videoflouroscopy and manometry, such as cricopharyngeal muscle hypertonicity or cricopharyngeal web. 2,3 Still, despite addressing targetable anatomic sites, dysphagia may persist, especially in the setting of multifactorial dysphagia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.