
Abstract

A 46-year-old man presented with a 5-year history of intermittent left cheek swelling after diet. Physical examination showed a 6-cm, soft, nontender swelling over the left parotid and pre-parotid region. A head and neck computed tomography scan revealed a left Stensen duct sialocele (Figure 1). He had received percutaneous incision and drainage at another tertiary medical center 2 years ago, but the issue soon recurred. Then intraoral incision and drainage was performed at the same center, but unfortunately, the procedure was again unsuccessful.
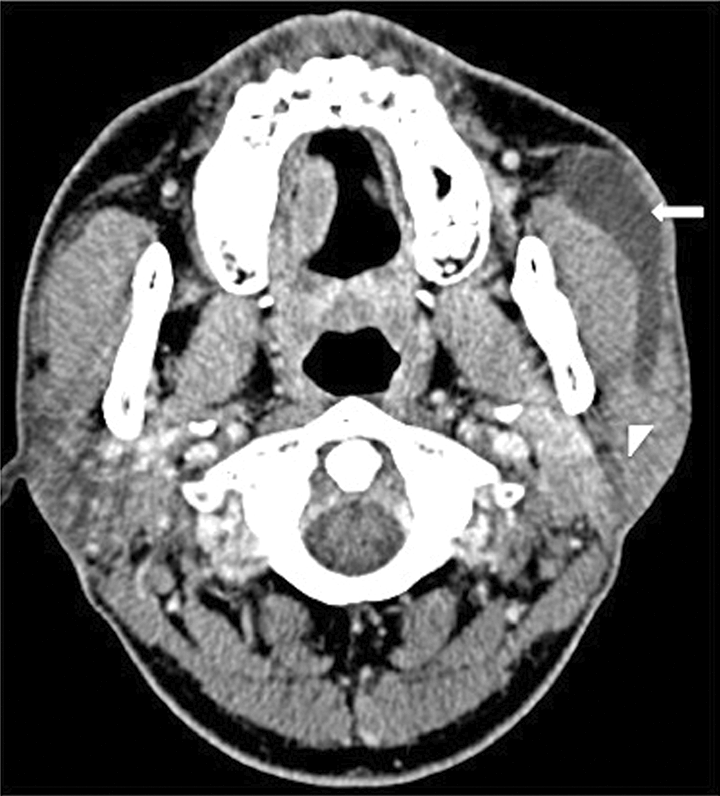
Computed tomogram of salivary gland showed recurrent sialocele over the left parotid gland (arrow head: left parotid gland, arrow: sialocele of Stensen duct).
Considering the previous unsuccessful standardized treatments, a surgical approach using sialendoscopy and stent insertion was planned and performed under general anesthesia. After semirigid scope insertion, one stricture site was noted near the papilla (Figure 2A). A sialocele was present behind the stricture site and extended 5.7 cm proximally from the stricture site. Figure 2B shows the successfully dilated stricture site under sialendoscopy. A silastic stent with 2.0-mm outer diameter was then inserted into the duct bypassing the sialocele with the assistance of guidewire insertion (Figure 2C). The stent was secured by 5-0 nonabsorbable sutures with the distal end protruding into the oral cavity (Figure 2D). The patient received postoperative antibiotics for 7 days.
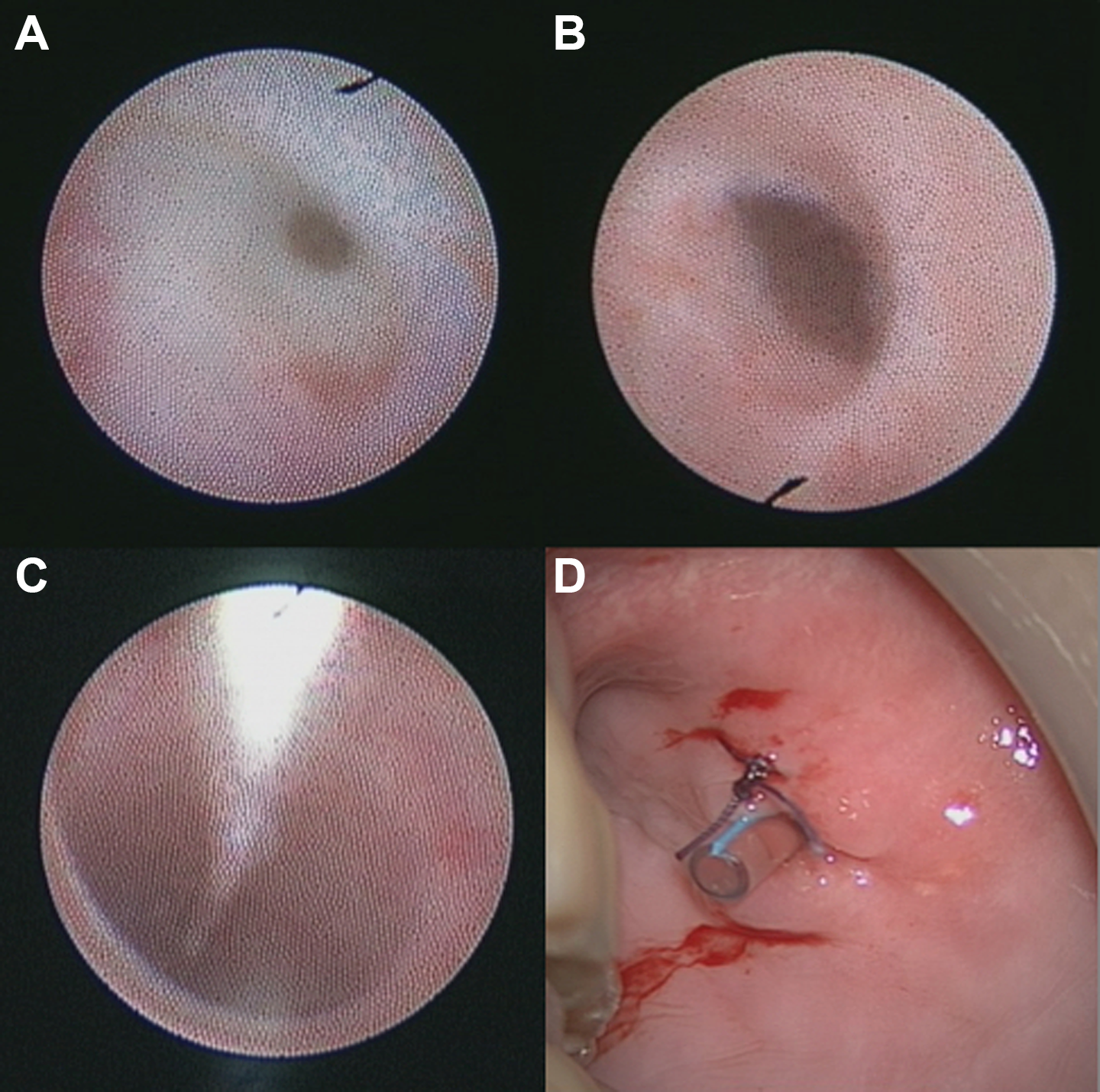
A, The ductal restenosis site during revised surgery. B, Successfully dilated ductal restenosis site. C, Guidewire insertion passing through the dilated sialocele lumen. D, The stent was secured by 5-0 nonabsorbable sutures with the distal end protruding into the oral cavity.
The facial swelling subsided in the first 2 weeks. However, after stent removal at 2 weeks, facial swelling was noted once again and persisted 1 month after the procedure. Thus, a revision sialendoscopy surgery was planned. The previous stricture site was still noted distal to the sialocele. The feeding tube stent was again inserted to bypass the sialocele (plastic 8F NG feeding tube, 2.667 mm). This time, the stent was kept for 4 weeks before removal, and the patient was checked regularly for 15 months without recurrences.
The pathophysiology of sialocele is mostly due to an injury to the duct or gland, which causes extravasation. Duct stricture is a common sign of post-trauma healing process. Currently, ductal dilations under sialendoscopy were reported to be an effective and simple way in managing salivary duct strictures with a successful rate up to 81%. 1 We inserted a stent to bypass the stricture site. The stent reduces sialocele input by bypassing the salivary flow to the extravasation site, which allowed the ductal mucosa to heal in a stable environment without flow. In this report, we describe a Stensen duct sialocele treated successfully by sialendoscopy without recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.