
Abstract
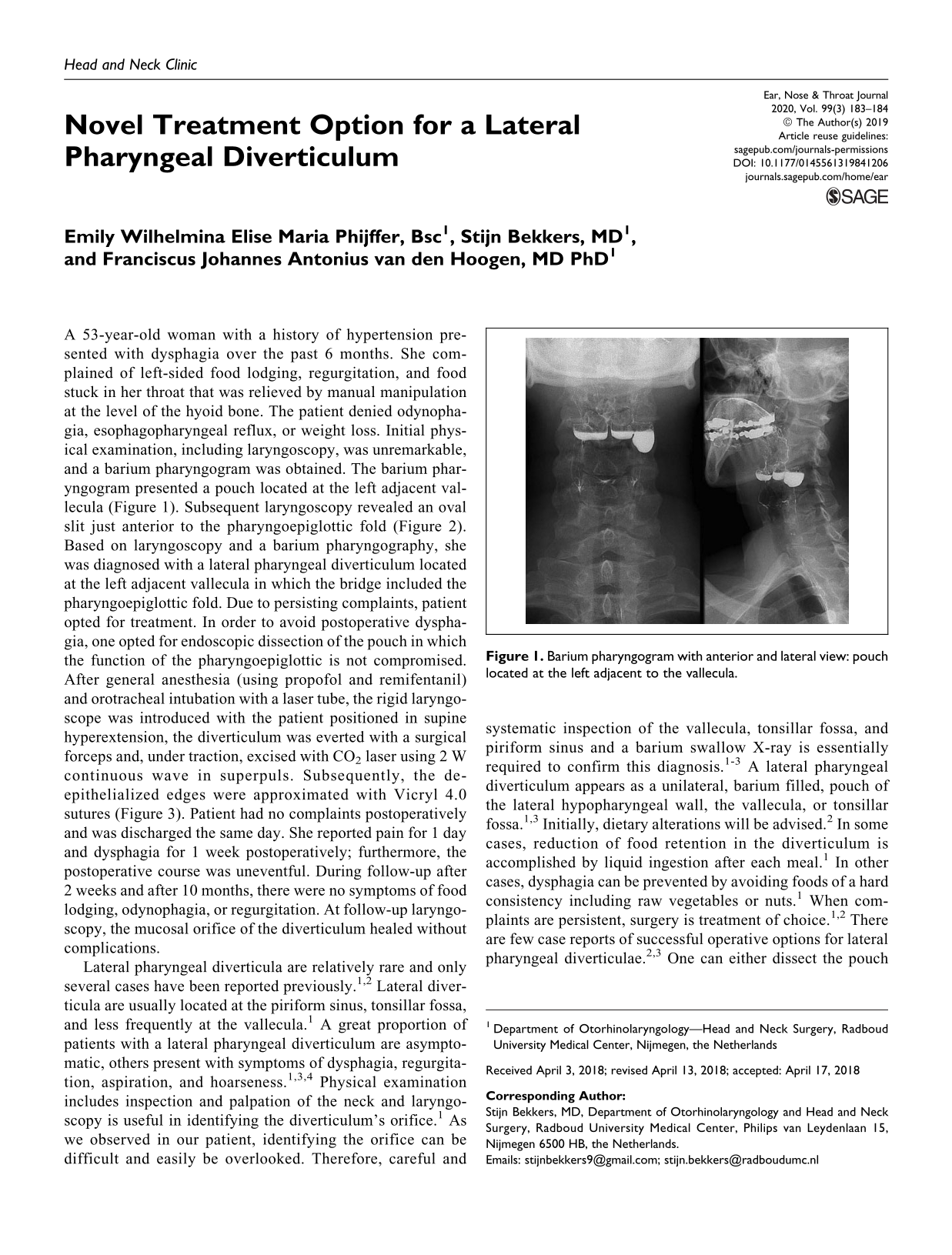
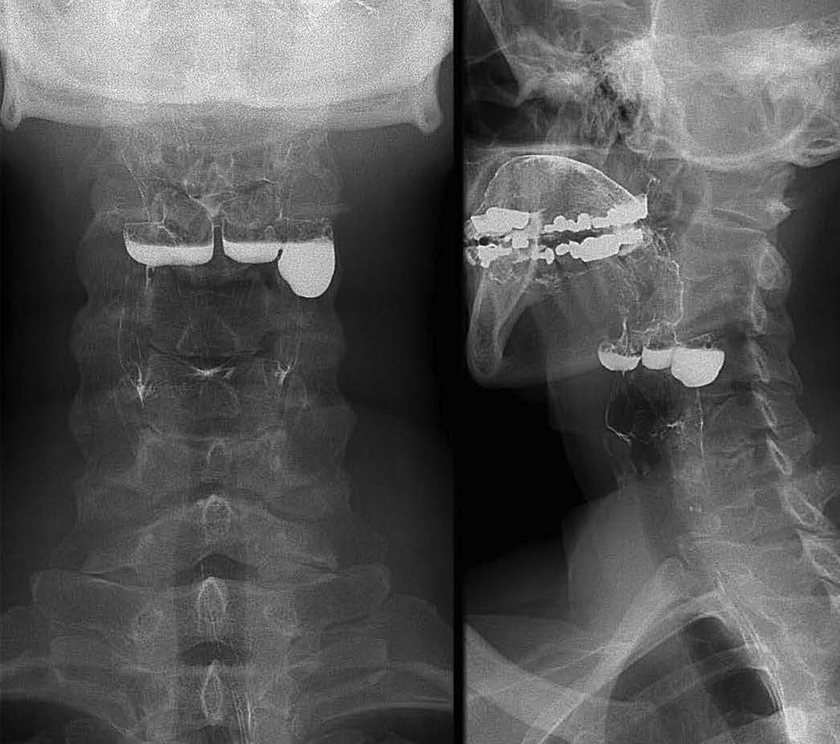
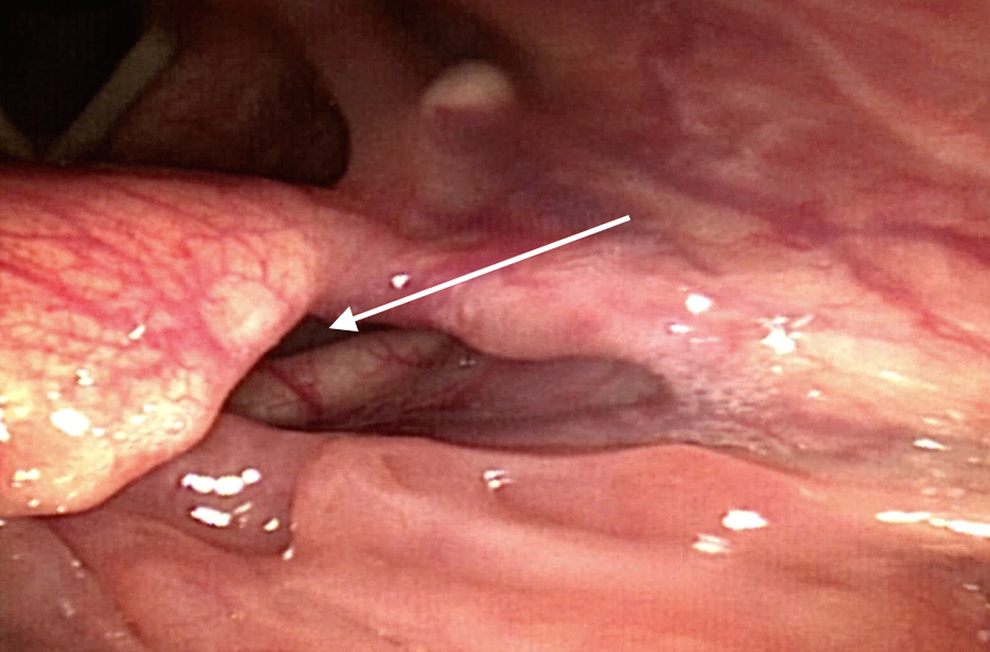
A 53-year-old woman with a history of hypertension presented with dysphagia over the past 6 months. She complained of left-sided food lodging, regurgitation, and food stuck in her throat that was relieved by manual manipulation at the level of the hyoid bone. The patient denied odynophagia, esophagopharyngeal reflux, or weight loss. Initial physical examination, including laryngoscopy, was unremarkable, and a barium pharyngogram was obtained. The barium pharyngogram presented a pouch located at the left adjacent vallecula (Figure 1). Subsequent laryngoscopy revealed an oval slit just anterior to the pharyngoepiglottic fold (Figure 2). Based on laryngoscopy and a barium pharyngography, she was diagnosed with a lateral pharyngeal diverticulum located at the left adjacent vallecula in which the bridge included the pharyngoepiglottic fold. Due to persisting complaints, patient opted for treatment. In order to avoid postoperative dysphagia, one opted for endoscopic dissection of the pouch in which the function of the pharyngoepiglottic is not compromised. After general anesthesia (using propofol and remifentanil) and orotracheal intubation with a laser tube, the rigid laryngoscope was introduced with the patient positioned in supine hyperextension, the diverticulum was everted with a surgical forceps and, under traction, excised with CO2 laser using 2 W continuous wave in superpuls. Subsequently, the de-epithelialized edges were approximated with Vicryl 4.0 sutures (Figure 3). Patient had no complaints postoperatively and was discharged the same day. She reported pain for 1 day and dysphagia for 1 week postoperatively; furthermore, the postoperative course was uneventful. During follow-up after 2 weeks and after 10 months, there were no symptoms of food lodging, odynophagia, or regurgitation. At follow-up laryngoscopy, the mucosal orifice of the diverticulum healed without complications.
Barium pharyngogram with anterior and lateral view: pouch located at the left adjacent to the vallecula.
Pharyngoscopy: the arrow shows an oval slit just anteriorly to the pharyngoepiglottic fold.
Postoperative result after excision with CO2 laser.
Lateral pharyngeal diverticula are relatively rare and only several cases have been reported previously. 1,2 Lateral diverticula are usually located at the piriform sinus, tonsillar fossa, and less frequently at the vallecula. 1 A great proportion of patients with a lateral pharyngeal diverticulum are asymptomatic, others present with symptoms of dysphagia, regurgitation, aspiration, and hoarseness. 1,3,4 Physical examination includes inspection and palpation of the neck and laryngoscopy is useful in identifying the diverticulum’s orifice. 1 As we observed in our patient, identifying the orifice can be difficult and easily be overlooked. Therefore, careful and systematic inspection of the vallecula, tonsillar fossa, and piriform sinus and a barium swallow X-ray is essentially required to confirm this diagnosis. 1 -3 A lateral pharyngeal diverticulum appears as a unilateral, barium filled, pouch of the lateral hypopharyngeal wall, the vallecula, or tonsillar fossa. 1,3 Initially, dietary alterations will be advised. 2 In some cases, reduction of food retention in the diverticulum is accomplished by liquid ingestion after each meal. 1 In other cases, dysphagia can be prevented by avoiding foods of a hard consistency including raw vegetables or nuts. 1 When complaints are persistent, surgery is treatment of choice. 1,2 There are few case reports of successful operative options for lateral pharyngeal diverticulae. 2,3 One can either dissect the pouch externally or dissect the bridge that separates the pouch from the lumen of the pharynx with laser surgery or stapler technique preventing food from lodging in the pouch. 3 Endoscopic dissection of the bridge is theoretically advocated due to a brief anaesthetic time, less extensive dissection, early oral intake, and less scarring for subsequent revision surgery when compared to external surgery. However, in case the diverticulum is located at the adjacent vallecula in which the bridge includes the pharyngoepiglottic fold, one should be reluctant of dissecting the bridge in order to avoid postoperative dysphagia. In conclusion, this case illustrates that endoscopic laser dissection is a novel, safe treatment option for lateral pharyngeal diverticula.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.