
Abstract
Asymmetrical tonsillar enlargement is a common referral to the ear, nose, and throat clinic, with the main diagnostic concern being oropharyngeal malignancy. 1 Approximately, 5% of patients with asymmetrical tonsillar enlargement will prove to have a malignancy with the most common histopathological subtypes being squamous cell carcinoma and lymphoma. 2,3 A differential diagnosis may be a parapharyngeal mass displacing the tonsil medially of which paraganglioma is a rare cause.
We demonstrate a rare case of paraganglioma presenting initially as recurrent tonsillitis with asymmetrical tonsillar enlargement.
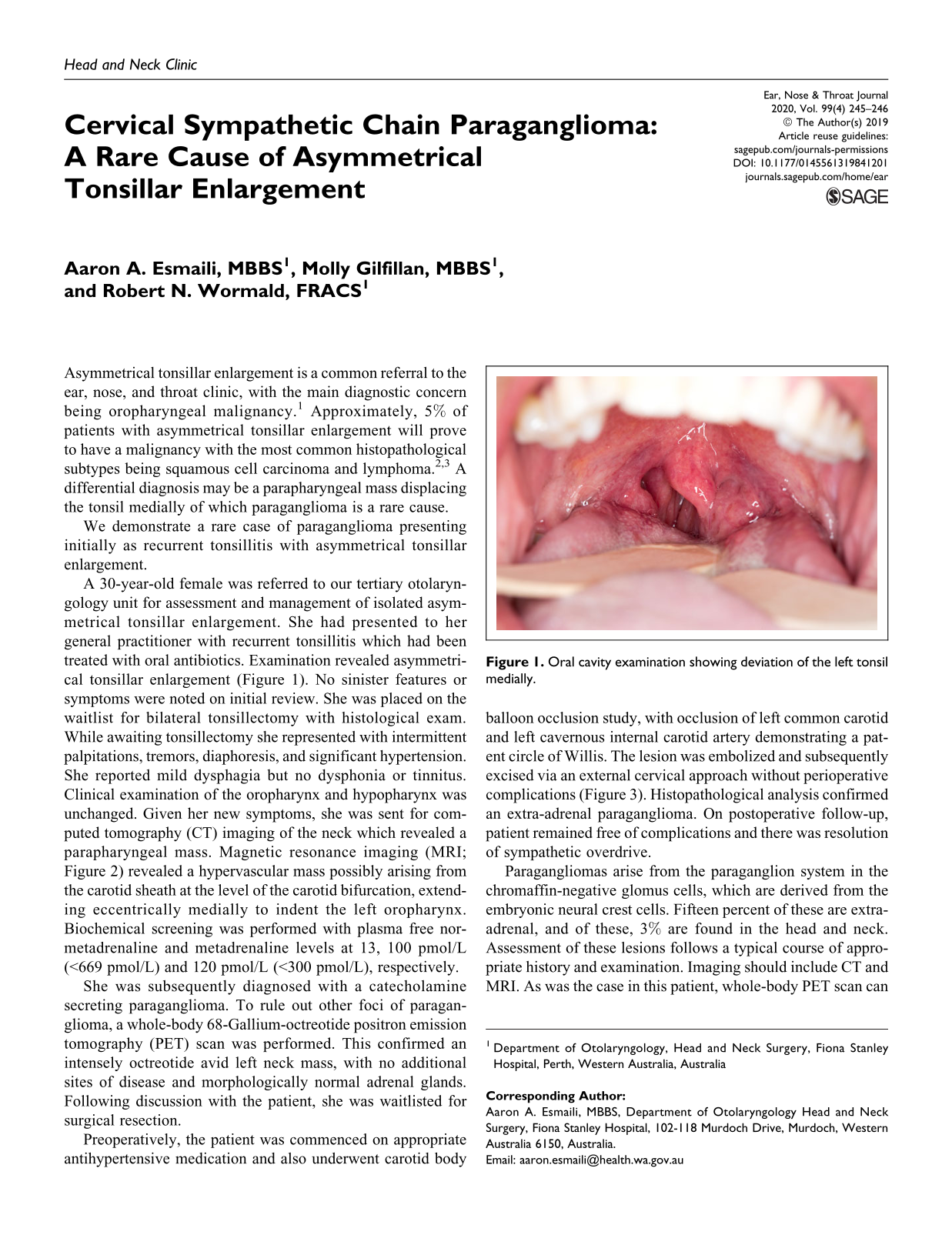
A 30-year-old female was referred to our tertiary otolaryngology unit for assessment and management of isolated asymmetrical tonsillar enlargement. She had presented to her general practitioner with recurrent tonsillitis which had been treated with oral antibiotics. Examination revealed asymmetrical tonsillar enlargement (Figure 1). No sinister features or symptoms were noted on initial review. She was placed on the waitlist for bilateral tonsillectomy with histological exam. While awaiting tonsillectomy she represented with intermittent palpitations, tremors, diaphoresis, and significant hypertension. She reported mild dysphagia but no dysphonia or tinnitus. Clinical examination of the oropharynx and hypopharynx was unchanged. Given her new symptoms, she was sent for computed tomography (CT) imaging of the neck which revealed a parapharyngeal mass. Magnetic resonance imaging (MRI; Figure 2) revealed a hypervascular mass possibly arising from the carotid sheath at the level of the carotid bifurcation, extending eccentrically medially to indent the left oropharynx. Biochemical screening was performed with plasma free nor-metadrenaline and metadrenaline levels at 13, 100 pmol/L (<669 pmol/L) and 120 pmol/L (<300 pmol/L), respectively.
Oral cavity examination showing deviation of the left tonsil medially.

Magnetic resonance imaging showing parapharyngeal tumor displacing the left oropharynx medially.
She was subsequently diagnosed with a catecholamine secreting paraganglioma. To rule out other foci of paraganglioma, a whole-body 68-Gallium-octreotide positron emission tomography (PET) scan was performed. This confirmed an intensely octreotide avid left neck mass, with no additional sites of disease and morphologically normal adrenal glands. Following discussion with the patient, she was waitlisted for surgical resection.
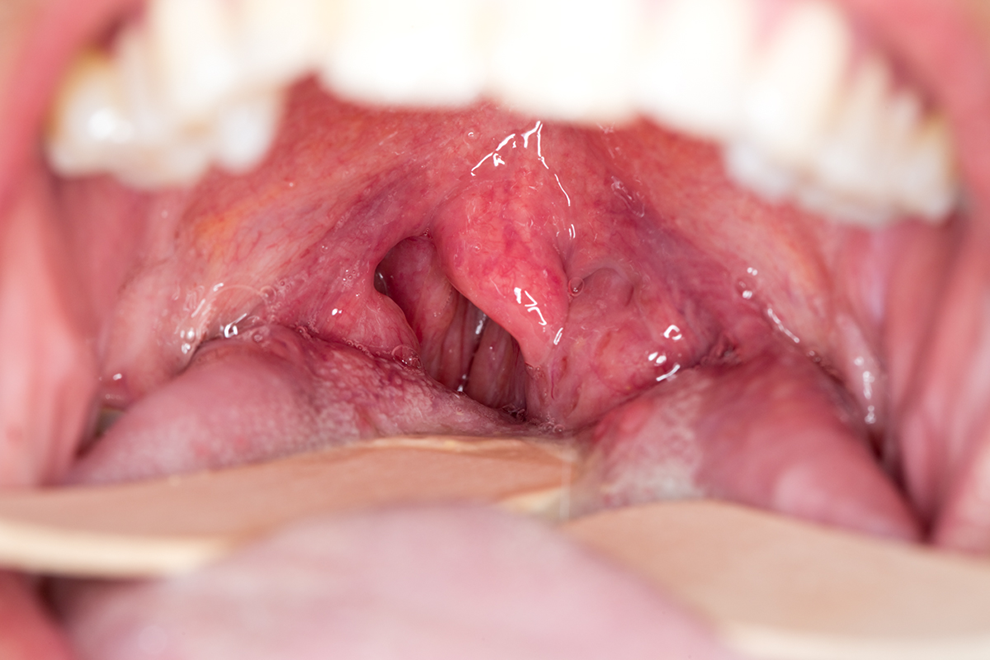
Preoperatively, the patient was commenced on appropriate antihypertensive medication and also underwent carotid body balloon occlusion study, with occlusion of left common carotid and left cavernous internal carotid artery demonstrating a patent circle of Willis. The lesion was embolized and subsequently excised via an external cervical approach without perioperative complications (Figure 3). Histopathological analysis confirmed an extra-adrenal paraganglioma. On postoperative follow-up, patient remained free of complications and there was resolution of sympathetic overdrive.
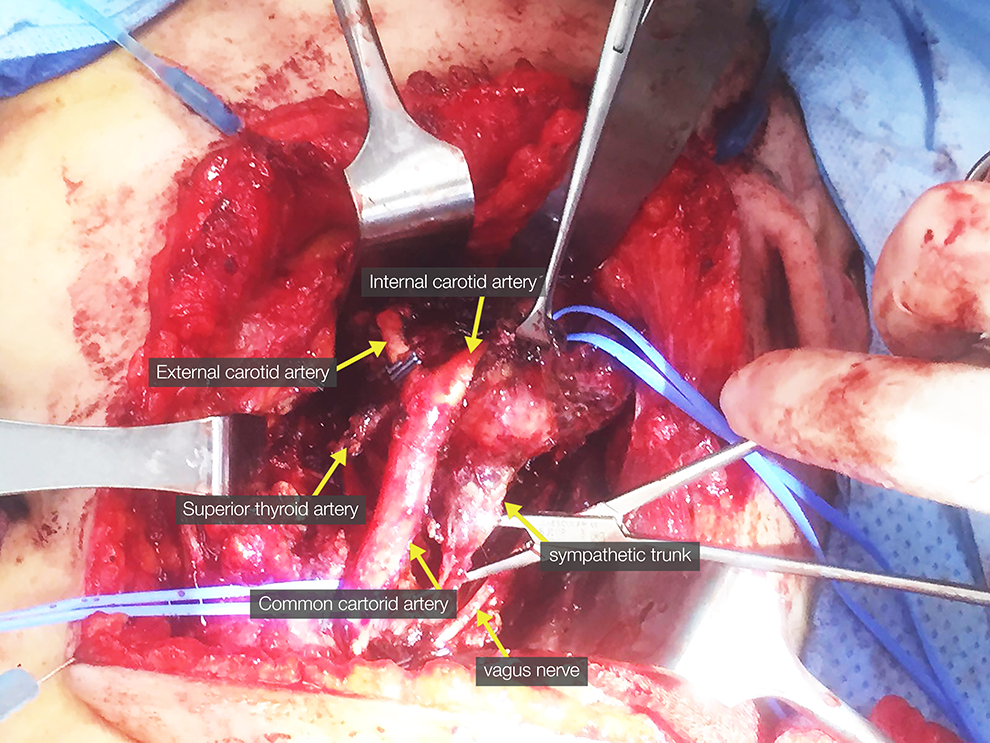
Intraoperative image of patient undergoing resection of the sympathetic chain paraganglioma.
Paragangliomas arise from the paraganglion system in the chromaffin-negative glomus cells, which are derived from the embryonic neural crest cells. Fifteen percent of these are extra-adrenal, and of these, 3% are found in the head and neck. Assessment of these lesions follows a typical course of appropriate history and examination. Imaging should include CT and MRI. As was the case in this patient, whole-body PET scan can be utilized to confirm the absence of other paraganglionic foci given secreting tumors of the head and neck are rare and usually arise from the abdomen. 4 Management options include observation, radiotherapy, and surgical resection. 5 Surgical resection may be indicated in patients with relatively smaller tumors, younger age, secreting lesion, significant local mass effect, and tumor progression after radiation. 5 Studies have shown that resection can result in up to 100% local control, with larger tumors showing a greater risk of postoperative neurovascular complications. 6,7 The above patient was young and otherwise fit, with a relatively large tumor which was actively secreting metadrenaline causing sympathetic overdrive. She therefore underwent embolization of the lesion with subsequent definitive surgical resection.
This case highlights paraganglioma as a rare differential diagnosis for unilateral tonsillar enlargement. Further clinical evaluation revealed symptoms of sympathetic overdrive and subsequent imaging led to the diagnosis of a paraganglioma. This report therefore highlights the need for sound clinical assessment and subsequent use of appropriate biochemical analysis and radiological imaging in the setting of asymmetrical tonsillar enlargement to help differentiate the cause. In the presence of symptoms consistent with a secreting tumor, imaging of the neck is essential.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.