
Abstract
A tracheotomy is a basic operation for the otorhinolaryngologist. According to reports from the United States and from our experience, there has been a steady decline in the number of tracheostomies performed by young resident doctors. Due to concerns for inadequate training of young residents, we developed a tracheotomy course consisting of a lecture, a live animal model, and questionnaires. The aim of this study was to evaluate the effectiveness of this training model. Twelve volunteer resident doctors joined the training course and, following a lecture by a senior surgeon, practiced tracheostomies with a 4-month-old female swine weighing 32 kg. We recorded the procedure time, blood loss, and complications. The doctors’ procedural competence was recorded using questionnaires before and after the training. All operations were completed within 30 minutes, and the blood loss was less than 5 ml. There were no serious acute complications. After the training, young residents had improved scores on surgical landmark recognition, overall procedural competence, confidence in performing the procedure, and understanding of the surgical procedures and equipment (P < .05). Our findings reveal that an animal model-based tracheotomy course is an effective training model for young resident doctors.
Keywords
Introduction
When a patient presents with upper airway obstruction or acute respiratory failure, establishing an artificial airway is essential. 1,2 The artificial airway is established primarily by endotracheal intubation or tracheotomy. Endotracheal intubation can be performed by a transoral or transnasal approach, which are quick and easy methods for patients in an emergency situation. 1 In general, orotracheal intubation is more convenient but can cause more discomfort for the patient compared to nasotracheal intubation. 3 On the other hand, nasotracheal intubation is technically more difficult, and the diameter of the tracheal tube is smaller, which can increase the airway resistance and the work of breathing. 2
However, prolonged endotracheal intubation may increase the occurrence of side effects, such as ventilator-associated pneumonia and subglottic stenosis. Therefore, a tracheotomy is appropriate when the patient is on a ventilator for more than 10 days and unable to be weaned off, has an upper airway obstruction, cannot effectively cough to evacuate secretions, or requires airway protection (including cases of stroke and traumatic neurologic insult). 4,5
A tracheotomy is a historic and basic operation for otorhinolaryngologists. 6 The procedure begins with a skin incision, followed by subcutaneous tissue separation, strap muscle separation, thyroid traction, tracheal wall incision, and finally, tracheal tube insertion. 7 Young residents typically practice this procedure under the supervision of senior surgeons. 8 In recent years, due to the increasing emphasis on patient safety and changes to the health-care system, a policy of operating first on animals before applying the procedure to patients is often considered. 9 A prior study has shown that practicing on animal models allows physicians to become familiar with cricothyroidotomy. 10 From our experience and reports from the United States, we found that exposure to tracheotomy for otorhinolaryngology residents has been declining, and residents perform fewer tracheostomies each year. 11 Due to concerns for inadequate training of young residents, we developed an animal model-based tracheotomy course.
We used live swine models to compare preferential techniques for skin and tracheal wall incisions and found no significant differences in the preferences for horizontal and vertical skin incision techniques, as well as horizontal tracheal wall incision and window creation techniques. 12 Therefore, we used the traditional vertical skin incision and tracheal wall window creation for this tracheotomy course to simulate the actual procedure on humans. The aim of this study was to evaluate the effectiveness of this training model.
Patients and Methods
This study was approved by the Research Ethics Committees of the hospital where the study took place (IACUC-2017-FEMH-07). We recruited young residents from different hospitals to undergo the tracheotomy course. In this training model, the senior physician first gave a lecture and demonstrated the entire procedure and surgical equipment. Subsequently, young residents practiced performing the tracheotomy using the live swine model.
We used four 4-month-old female swine weighing 32 kg. These swine underwent general anesthesia. First, the veterinarian performed orotracheal intubation (internal diameter 5 mm) with the swine in the prone position. The swine was then fixed in the supine position on the operating table with assisted ventilation using the endotracheal tube. The veterinarian controlled the level of general anesthesia. The residents were randomly allocated to 1 of 4 groups. Each group consisted of 3 young residents and 2 experienced nurses in an operating room. One doctor performed the operation, while the other 2 doctors were first and second assistants. The tracheotomy practice began with the first 2 groups (group A and group B) simultaneously, followed by the second 2 groups (group C and group D). The procedure was initiated with a vertical skin incision, followed by subcutaneous tissue and strap muscle separation, thyroid traction, tracheal wall window creation (Figure 1), and finally, tracheal tube insertion, simulating the routine practice in humans. Thirty minutes after the procedure, the swine was euthanized.

Tracheotomy with tracheal wall window creation. After exposure of the tracheal wall, the residents perform tracheal wall window creation. The endotracheal tube is gradually removed, and the tracheotomy tube is inserted to complete the procedure.
We recorded the procedure time from skin incision to endotracheal tube insertion, total blood loss, and complications. The doctors’ competence for the operation was recorded with questionnaires before and after the training. The questionnaires were modified from those of a previous study 13 and included ratings on ease of landmark recognition and ease of overall procedure on a 10-point scale (0: very easy, 10: very difficult). Confidence in performing the surgery and an understanding of the surgical procedures and equipment were evaluated on a 5-point scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). We also recorded the residents’ experiences during the animal tracheotomy model, and residents were asked whether or not they would recommend this workshop for other residents in the future.
Scores from the questionnaires were expressed as means and standard deviations. Wilcoxon signed-rank tests were used to compare the doctors’ competence before and after the training course. We also compared the improvement in competence depending on whether or not the resident had any previous experience in animal model surgeries. Statistical analysis was carried out using STATA software, version 12.0 (Stata Statistical Software: Release 12. College Station, Texas: Stata Corp LP).
Results
A total of 12 residents (2 females and 10 males) participated in this study. The average age of the participants was 26.5 years old. There were 9 postgraduate year 1 residents and 3 interns. Five (41.67%) doctors had previous experience performing animal model surgeries. Five (41.67%) doctors had previous experience performing tracheostomies, but all less than 5 times.
The outcomes of the operation for each group are shown in Table 1. All operations were completed within 30 minutes, and the blood loss was no more than 5 mL. There were no serious acute complications, such as massive wound bleeding, subcutaneous emphysema, or pneumothorax.
The Results of the 4 Participant Groups in the Swine Tracheotomy Training Model.a
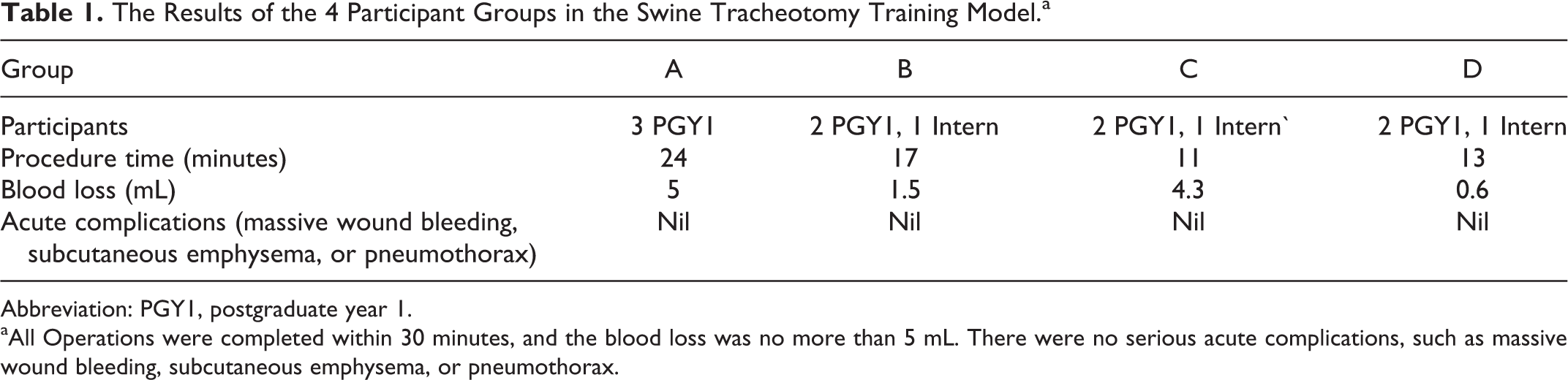
Abbreviation: PGY1, postgraduate year 1.
aAll Operations were completed within 30 minutes, and the blood loss was no more than 5 mL. There were no serious acute complications, such as massive wound bleeding, subcutaneous emphysema, or pneumothorax.
The results of the questionnaires are shown in Table 2. After the training course, there were significant improvements in the scores for ease of landmark recognition, ease of the overall procedure, confidence in performing the procedure, and understanding the surgical procedures and equipment (P value < .05). Residents without previous experience in animal model surgery had significant improvements in the scores for ease of landmark recognition, ease of the overall procedure, confidence in performing the procedure and understanding of surgical procedures and equipment (P value < .05). Residents with previous experience in animal model surgeries had significant improvement in the understanding of surgical procedures (P value < .05; Table 3). Nine (75%) of the 12 participants stated they would recommend other residents for the workshop, and the remaining 3 doctors did not provide a response to this question.
The Results of the Questionnaires (Pre-Operation and Post-Operation Assessments in a Total of 12 Participants).a
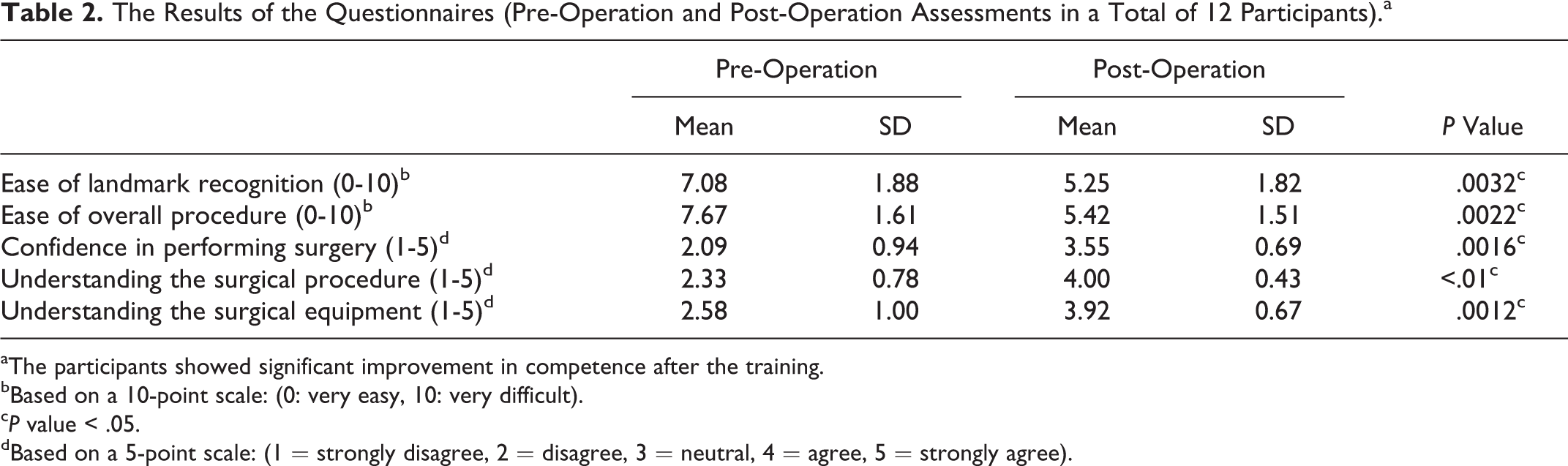
aThe participants showed significant improvement in competence after the training.
bBased on a 10-point scale: (0: very easy, 10: very difficult).
c P value < .05.
dBased on a 5-point scale: (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree).
The Improvement in Competence Based on the Residents’ Previous Experience in Animal Model Surgery.
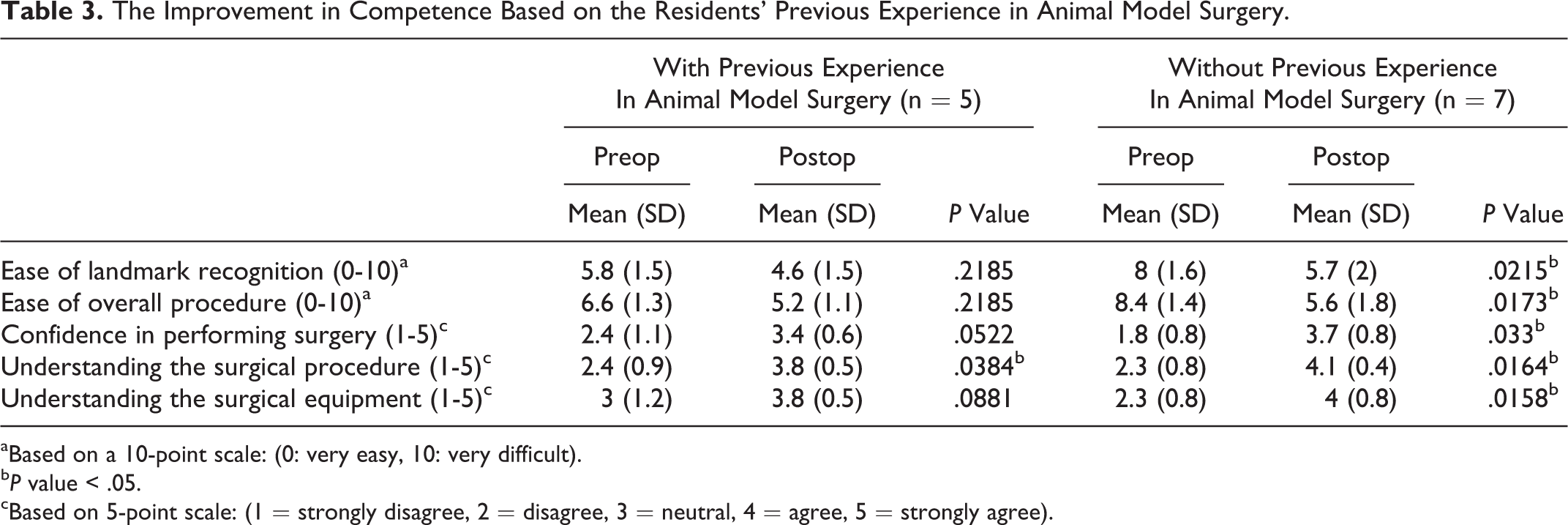
aBased on a 10-point scale: (0: very easy, 10: very difficult).
b P value < .05.
cBased on 5-point scale: (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree).
Discussion
We found that the live animal model-based tracheotomy course is an effective training model for young resident doctors.
Live Animal Model Training
Otorhinolaryngology residents are often at the forefront for managing acute airway conditions. Proper training with lectures and simulations is a safe method to learn such skills and may improve the residents’ competence in the clinical setting. In addition to the experiences in the United States 11 , according to a survey study in Canada, 14 otorhinolaryngology residents reported inadequate training on advanced airway management. They also noted less teaching time using simulations and cadaver or animal models compared to didactic lectures or learning in the operating room. Thus, we aimed to develop a training model for airway management.
A previous porcine model for cricothyroidotomy was well-accepted among medical students and residents. 10 Because elective tracheotomy is commonly performed, there is also a need for adequate tracheotomy training.
Other institutions have used cadaver models for tracheotomy practice, 15 which can also be a good training model. However, the cadavers lack skin compliance and blood circulation and thus are unable to simulate all physiologic conditions of a live human. A specific preparation for cadaver preservation is also required. 9 Based on the above reasons, we developed a live swine model for tracheotomy training.
Easy Learning and a Low-Risk Method
Differences in procedure time were observed between the 4 resident groups (Table 1). The overall procedure durations of groups C and D were shorter than those of groups A and B. This may be because groups A and B performed the tracheotomy first, and groups C and D stood nearby and observed the entire procedure. Therefore, in addition to the lecture, the residents in groups C and D had the opportunity to observe the entire procedure, which may have allowed them to complete the procedure in a shorter duration. This suggests that the live swine tracheotomy model is an easy way to learn.
Young residents can also learn the possible complications and management of such complications from the live animal tracheotomy model. 9 In this study, there were no serious acute complications, such as massive wound bleeding, subcutaneous emphysema or pneumothorax. These results show that an animal-based tracheotomy model is a low-risk environment to practice tracheostomies for young residents.
Improvement of Surgical Competence
After the training, the residents without previous experience in animal model surgery had significant improvement in greater number of items on the questionnaires compared to those with previous animal model surgery experience (Table 3). These results show that a live swine tracheotomy model can improve the surgical competence of young residents, especially for those without previous experience in animal model surgery.
One study has compared the effectiveness of various cricothyroidotomy training models. 16 Volunteers were trained with either a live pig or a simulator (TraumaMan, Seattle, WA) and subsequently performed cricothyroidotomy on human cadavers. The success rate of cricothyroidotomy on the human cadaver was 75% in the animal model group and 53% in the simulator group, but there was no significant difference between the 2 groups due to a small sample size. These findings showed that animal model training not only improves surgical competence but also increases the success rate in future clinical practice.
Limitations
There are several limitations to this study. First, the anatomical structures of a swine are not the same as those of humans. For example, the thyroid is round in the swine but has 2 lobes in humans, and the skin compliance of a swine is not the same as that of humans. Therefore, it is not possible to fully simulate the anatomical structures of humans using a swine model. However, in our live animal model, it was possible to monitor physiologic reactions to the procedure and face possible complications such as acute bleeding. Second, the sample size was relative small due to the limitation of funding. Furthermore, residents who had previous experience using an animal surgery or tracheotomy model may have influenced the results. 17 Third, the swine were euthanized 30 minutes later, and therefore, there was a lack of long-term follow-up. We hope to continue our workshop and conduct long-term, large-scale studies to improve these shortcomings in the future.
Through this experience, we showed that an animal model-based tracheotomy course is an effective training method for young resident doctors. Through this animal model training, residents can learn in a low-stress environment 14 and become skilled in performing tracheostomies. This training model can ultimately help young residents become competent otorhinolaryngologists.
Footnotes
Acknowledgments
We would like to thank the doctors who volunteered to participate and the nurses who assisted with the operations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Far Eastern Memorial Hospital Program (FEMH-2017-C-043).