
Abstract
Large and deep defects resulting from lateral skull base surgery represent a challenge to the head and neck surgeon. Different microvascular free flaps have specific advantages and disadvantages. While the pedicled pectoralis major flap is considered a “work horse,” it comes with a rather short pedicle. The aim of this study was to analyze the vascular anatomy of the pectoralis major flap and assess its suitability for microvascular transfer. Anatomical studies have been performed on 6 Thiel-fixed cadavers allowing a harvest of 12 flaps by the same surgeon. Measurements of the pedicle’s length and vessel diameters have been taken with a ruler and caliper. The mean pedicle length and mean diameters (Ø) of the thoracoacromial artery and concomitant vein were found to be 9.8 cm, Ø 4.2 mm, and Ø 4.9 mm, respectively. These results suggest the potential utility of a free pectoralis major flap with microvascular anastomosis.
Introduction
After tumor resection, surgical reconstruction is needed to restore functional aspects and aesthetic integrity. Extensive defects represent a challenge to the head and neck surgeon, for example, in the area of the lateral skull base after petrosectomy. This procedure could be necessary for resection of tumors of the ear canal combined with total or radical parotidectomy. A well-established and widely used flap in head and neck surgery is the pedicled pectoralis major flap. 1 It was first described in 1979 by Ariyan and allows the transplantation of a large quantity of soft muscular tissue into the defect and affords an expansive skin paddle when necessary. Furthermore, its pedicle localization is highly reliable and the simplicity of closure technique for the primary donor site is advantageous. The pedicle’s length is considered the only major limitation of this versatile flap. 2 The use of “the” pedicled flap at the lateral skull base is impossible due to the limited pedicle length even if the flap is pulled through under the clavicle. 3 Thus, for bridging long distances, a microvascular free flap would be ideal. The well-known radial forearm free flap is easy to harvest but consists of fasciocutaneous tissue which hardly contains enough volume to fill the defect encountered after petrosectomy. Other musculocutaneous free flaps such as the anterolateral thigh flap or the rectus abdominis flap come along with smaller vessel diameters and force the head and neck surgeon to operate in regions far away from the primary surgical localization. 4,5 On the other hand, it could improve time of surgery if 2 teams are available for a simultaneous approach. Harvesting of the latissimus dorsi flap on the other hand makes it necessary to change the patient’s position during the operation or perform tumor resection and reconstructive surgery with the patient in semiprone position. Because of the frequent use of the pectoralis major flap in reconstructive head and neck surgery and its localization close to the site of interest with a reliable anatomy, a free harvest with microvascular anastomosis could be a solution. In this anatomical study, the cadavers were preserved using Thiel-fixation, an excellent method to retain the color and texture of organic material thus preventing shrinkage and induration. Through this method, we could obtain a more accurate measurement of the pedicle length compared to prior anatomical trials.
Patients and Methods
In order to analyze the pedicle of the pectoralis major flap, anatomical dissection of 12 flaps from 6 Thiel-fixed human bodies was performed. The study was approved by the institutional research ethics committee. The cadavers did not present any scars from previous surgery on the clavipectoral region ensuring the integrity of the harvested pedicle. The average age of the body donors, consisting of 3 men and 3 women, was 85.5 years.
First, the pectoralis major flap was designed and raised. After submuscular preparation, the pedicle’s thoracoacromial artery and vein were identified and dissected until reaching the origin from the axillary artery (AA; Figure 1).
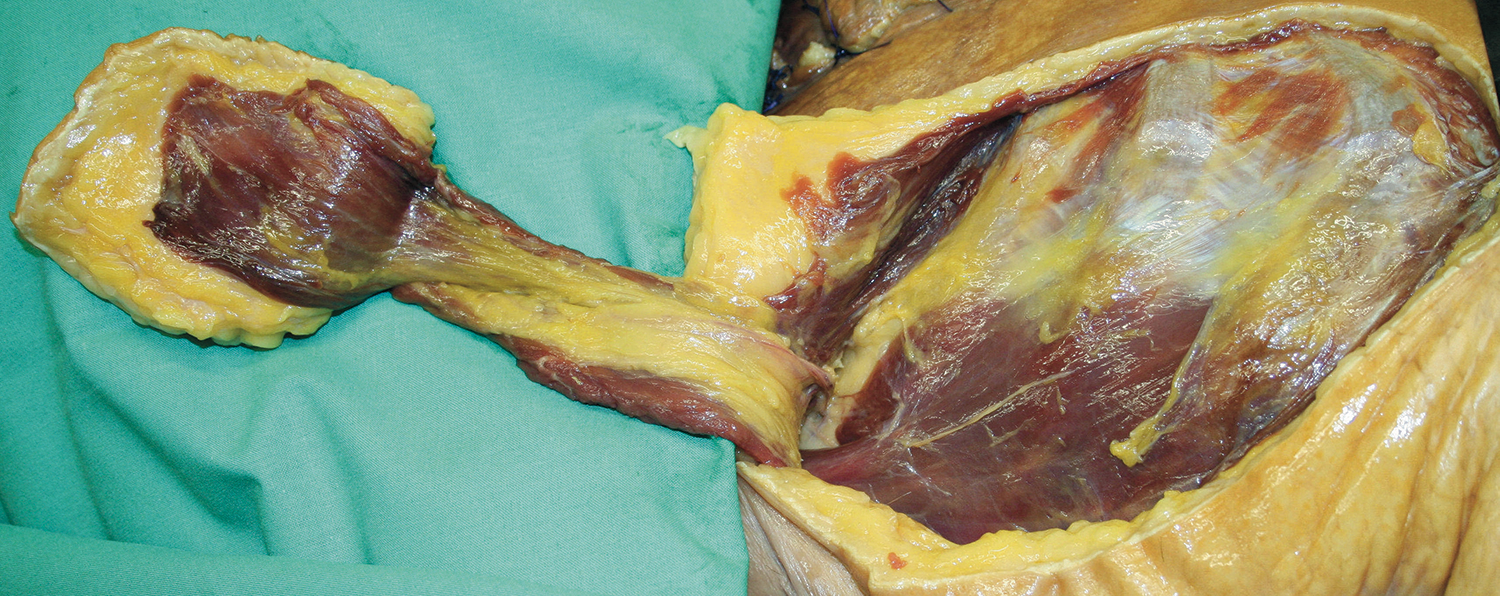
The image shows the pectoralis major flap raised from the right chest of a body donor analyzed for this study.
After further dissection in the clavipectoral triangle, all of the pertinent vessels were identified and marked with colored loops for photographic documentation (Figure 2).
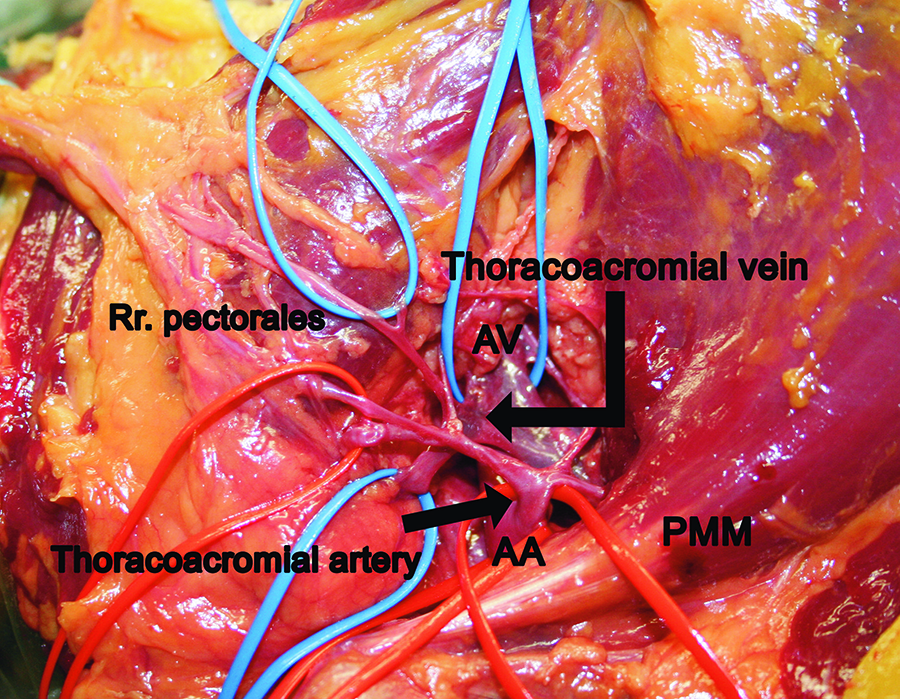
The photograph shows the dissected clavipectoral fossa with the pedicle vessels’ origin from the axillary artery (AA) and vein (AV), medial to the pectoralis minor muscle (PMM).
The thoracoacromial artery and vein were cut from the AA, dissected from surrounding tissue, and the flap harvested. For the determination of pedicle length, the entire span of the skeletonized thoracoacromial artery and vein was measured from its AA and axillary vein origin, respectively, to its entry inside the pectoralis major muscle. If the vessels branched before entering the muscle, the point of branching was used to measure the pedicle’s length. The internal diameter of the vessels was evaluated with a compass and ruler, and the measured values were confirmed with a caliper.
Results
In the 12 flaps harvested from the 6 body donors, the mean pedicle length was found to be 9.8 cm (Table 1).
Pedicle length in cm of each specimen (n = 12).
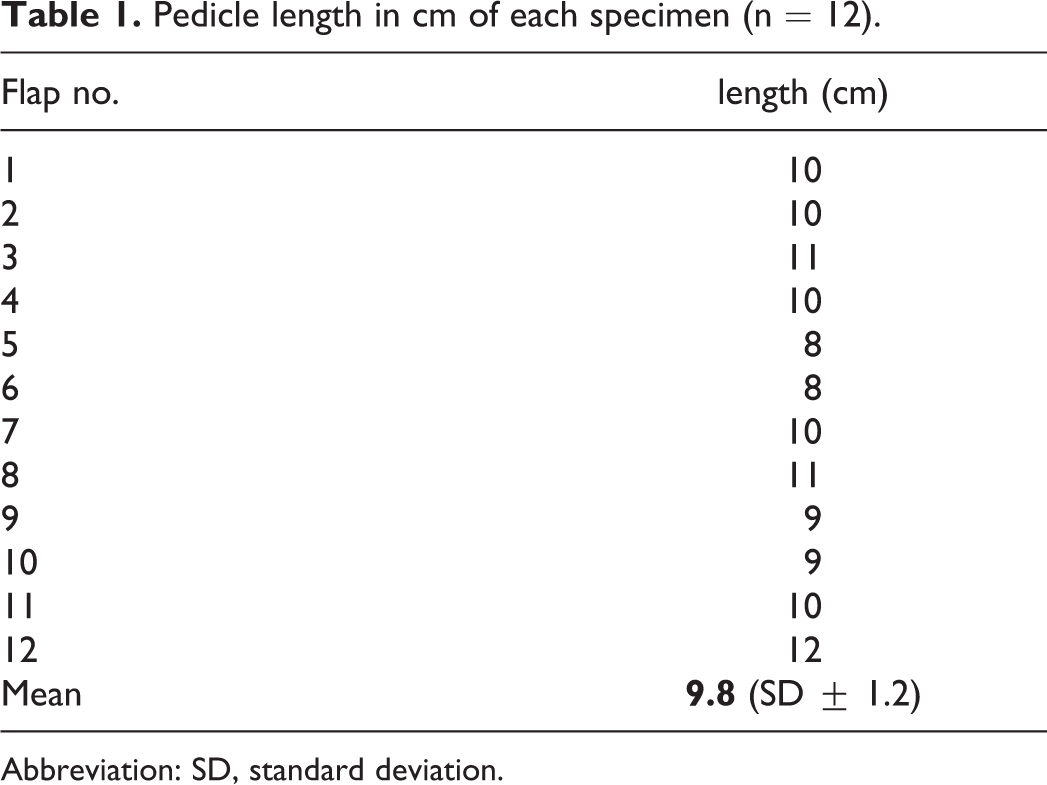
Abbreviation: SD, standard deviation.
Table 2 reports the diameter of the thoracoacromial artery (mean diameter 4.2 mm) and the concomitant thoracoacromial vein (mean diameter 4.9 mm) for each specimen.
Diameters of thoracoacromial artery and vein for each of the 12 flaps.
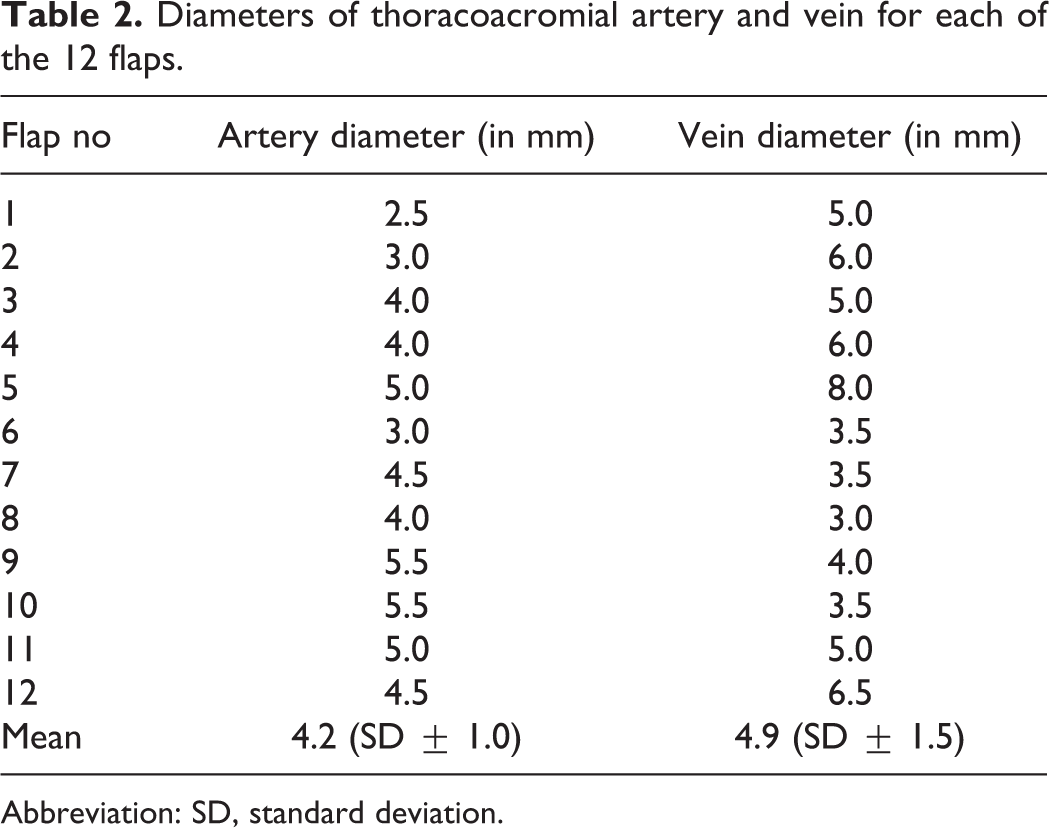
Abbreviation: SD, standard deviation.
Discussion
The pedicled pectoralis major flap is a reliable option for routine reconstruction of the floor of the mouth and base of the tongue as well as deeper cutaneous defects of the neck. With the maximum of rotation, it reaches the parotideal area. However, the limited range of pedicle rotation prevents its use in the lateral skull base. When considering the relatively reliable course of the pedicle vessels and the diameters evaluated in this study, it appears a variation of a microvascular pectoralis major free flap may be a valuable solution.
Zhang et al analyzed the free pectoralis major flap in 11 rats by taking the deep muscular part and the axillary vessels. After 72 hours, 9 of 11 flaps were still perfused. 6 Brunelli et al also performed the free pectoralis major flap in rats. When anastomosis of the thoracoacromial vessels failed because of the small diameters, they connected the axillary vessels to the recipients; 9 of 10 flaps survived. 7
The first description of a microvascular pectoralis major free flap in human patients appeared in 1976 in China and Japan for limb reconstruction. 8,9 In 1986, Reid et al performed the first microvascular pectoralis major free flap transfer to the head and neck region by raising the clavicular part of the muscle for intraoral reconstruction in 4 cases; in 1 patient, the authors also harvested the vascularized clavicular bone together with the flap for reconstruction of the lower leg. 10 Later use of the clavipectoral portion of the pectoralis major as a free flap was described by Seikaly et al in 1997 with the bony clavicula and in 2007 as merely a muscular flap. 11,12 In both articles, the authors consider the pedicle length to be a strongly limiting factor. In 2004, Yeh et al reported about 5 patients with failure of free flaps (3 anterolateral thigh flaps, 1 radial forearm flap, and 1 osteocutaneous fibula flap) after resection of oral cancer. Due to wound dehiscence and tissue necrosis after secondary reconstruction with pedicled pectoralis major flaps as salvage surgery, the authors performed a conversion into a microvascular free flap with anastomosis to the superficial temporal vessels to save the transplant. 13 Corten et al performed anatomical studies on 17 donor sites of formalin-fixed cadavers in 2006 and found the pedicle’s length to be 6.6 cm and the arterial diameter 1.8 mm. 14 Previous anatomical studies performed by Manktelow et al in 1980 showed similar arterial diameter values (1.5-2.1 mm) for 15 cadaver dissections of the sternocostal part of the muscle. 15 Later, in 2009, Corten et al performed 5 segmental pectoralis major free flaps in head and neck patients by raising the sternocostal part of the muscle; 4 of these flaps were successful in a long-term setting. 16 The use of a complete pectoralis major flap for the microvascular anastomosis technique has been described by Hallock in 2013 for reconstruction of a large cutaneous defect in the groin area of an obese patient. 17
In contrast to other studies, we established the values of vessel diameter and pedicle length on Thiel-fixed cadavers. The advantage of this fixation method is the elimination of shrinkage or enlargement of vasculature and other anatomical structures. 18 Thiel fixation is a very well-known and widely used method of conservation, especially for operation courses on human cadavers for medical doctors and dentists. 19,20 Previous anatomical studies have been performed on formalin-fixed cadavers with a certain rate of tissue shrinkage. 14 Since 2006, there have been no further anatomical cadaveric studies for the vascular supply of the pectoralis major flap. It should be noted that the vessels have been cut off and measured directly from their origin of the AA in this study, whereas in other studies, the pedicle has been resected at the medial border of the pectoralis minor muscle 14 or was not specified. 15 As the thoracoacromial trunk shows a larger diameter before splitting into 2 branches, this offers a larger vessel diameter for anastomosis. Furthermore, it increased the pedicle length, which may offer the possibility to anastomose the flap to lower branches of the external carotid artery rather than the temporal artery. The arterial supply to the shoulder originating from the thoracoacromial trunk must be resected to harvest the free pectoralis major flap in the described manner. However, the blood supply of the shoulder is given by natural anastomoses with the humeral circumflex vessels.
In head and neck surgery, certain regions can represent extended defects challenging to reconstruct after wide tumor resection, especially large defects of the lateral skull base resulting from simultaneous parotidectomy and petrosectomy. The skin flap used to cover the defect zone should be sufficiently large, while the soft tissue should be voluminous enough to bring well-perfused material into the wound base. The pedicled pectoralis major flap is not always suitable because of the long distance to be covered from the clavipectoral area to the skull base. However, the commonly used microvascular free flaps also present many disadvantages for the head and neck surgeon. The results of this study suggest the use of a microvascular pectoralis free flap for this particular purpose. Considering these results demonstrate a reliable and relevant diameter for the recipient vessels in vivo transplantation seems feasible. This study should encourage reconstructive surgeons to consider the free pectoralis major flap more frequently for the indications presented herein.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Acknowledgments
The authors want to thank the Institute of Anatomy and Cell Biology, Ulm University, Albert-Einstein Allee 11, 89081 Ulm, Germany, especially the director Professor MD Tobias M. Böckers, MD Ulrich Fassnacht, and Ernst Voigt for their valuable collaboration enabling this anatomical study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.