
Abstract
The objective of this study is to investigate the dimensional and volumetric measurements in the thyroarytenoid (TA) muscle in men and women using magnetic resonance imaging (MRI). The hypothesis is that there is a gender-related difference in these measurements. A retrospective chart review of 76 patients who underwent MRI of the neck at the American University of Beirut Medical Center was conducted. The dimension and volume of the right and left TA muscle were measured on axial and coronal planes short tau inversion recovery images. Male and female groups were compared with respect to demographic data and MRI findings using parametric and nonparametric tests. The mean length of the thyro-arytenoid muscle in males was larger than that in females on the right (males 2.44 [0.29] cm vs females 1.70 [0.22] cm) and on the left (males 2.50 [0.28] cm vs females 1.72 [0.24] cm) reaching statistical significance (P < .001). The mean width of the thyro-arytenoid muscle in males was larger than that in females on the right (males 0.68 [0.13] cm vs females 0.59 [0.11] cm) and on the left (males 0.68 [0.12] cm vs females 0.57 [0.12] cm) reaching statistical significance (P < .001). The mean height of the thyro-arytenoid muscle in males was larger than that in females on the right (males 1.05 [0.21] cm vs females 0.95 [0.12] cm) and on the left (males 1.05 [0.21] cm vs females 0.95 [0.12] cm) reaching statistical significance (P < .01 on the right and P < .05 on the left). The volume of the thyroarytenoid muscle in males was larger than that in females on the right (males 0.86 [0.25] mL vs females 0.48 [0.15] mL) and on the left (males 0.89 [0.27] mL vs females 0.48 [0.17] mL) reaching statistical significance (P < .001). The results of this investigation clearly indicate a significant difference in these measurements between men and women.
Introduction
Gender-related differences in the human voice are obvious with men having a considerably lower speaking fundamental frequency (F0) compared to women. 1,2 Although these differences are prominent during adolescence and throughout life, little is known about sexual dimorphism in relation to volumetric measures of the intrinsic laryngeal muscles, in particular vocal fold muscles. Patterns of sexual dimorphism have been previously reported in limb muscles indicating that men have larger fiber cross-sectional area and higher ratio of fast twitch fibers than women. 3 –5 These findings can hardly be generalized to include the intrinsic laryngeal muscles in view of the disparities in innervation, function, and contractile properties between the 2. 6 For instance, type 1 muscle fibers primarily involved in tonic contraction are predominantly present in muscles of the lower extremities whereas type 2 fibers with moderate resistance characterized by endurance predominate in laryngeal muscles. 7 –9
Learning about the volumetric measures of the vocal fold muscles carries important clinical implications in the understanding and treatment of vocal fold disorders. Most of the current literature on gender-related anatomical variations in the laryngeal structures is derived from either cadaveric, stereo-endoscopic, or imaging studies using plain radiographs, computerized tomographic images, or magnetic resonance imaging (MRI). 1 –6,10 –18 Magnetic resonance imaging in particular has been primarily used to investigate the relationship of the vocal tract with the cranio-cervical structures, the morphologic changes that occur during transition between vocal registers while singing, and the interplay between pitch alteration and laryngeal configuration. 19 –21 No prior study using MRI has been used for linear or volumetric measurements of the vocal folds despite the superiority of this imaging technique in soft tissue measurements in comparison with computed tomography (CT). 20,21
Given the scarcity of radiological reports on gender-related volumetric measurements of the vocal folds and given the paramount impact of these findings in phonosurgery, the authors of this article have investigated the dimensional and volumetric differences in the vocal fold thyroarytenoid (TA) muscle in men and women using MRI. The hypothesis is that there is a gender-related difference in TA muscle dimensional and volumetric measures on MRI.
Materials and Methods
After obtaining the approval of the institutional review board, a retrospective chart review of patients who underwent MRI of the neck at the American University of Beirut Medical Center during a period of 5 years (2010-2015) was conducted. Exclusion criteria included history of myopathy, vocal cord paralysis, laryngeal lesions or cancer, and laryngeal surgery or radiation. Patients with distorted imaging due to motion or other artifacts such as blurring or pixilation were also excluded.
Neck MRIs were of 4-mm slice thickness and performed using a 3.0 T Philips Ingenia (Andover, Massachusetts) machine. 22 The dimension and volume of the right and left TA muscle were measured on axial and coronal planes short tau inversion recovery images. In particular, the TA muscle vertical height was measured from its superior to inferior edge on coronal view, taking into account the longest visible height of the muscle. The anteroposterior length and width were measured on axial view, namely length was measured from the anterior commissure to the vocal process of the arytenoid cartilage and width from the medial to the lateral edge at mid-aspect of the muscle. The volume on the other hand was calculated by multiplying height, length, and width measurements. 22 Note that these measurements were made visually taking into account the lateral and cephalic extension of the TA muscle, see Figure 1A and B.
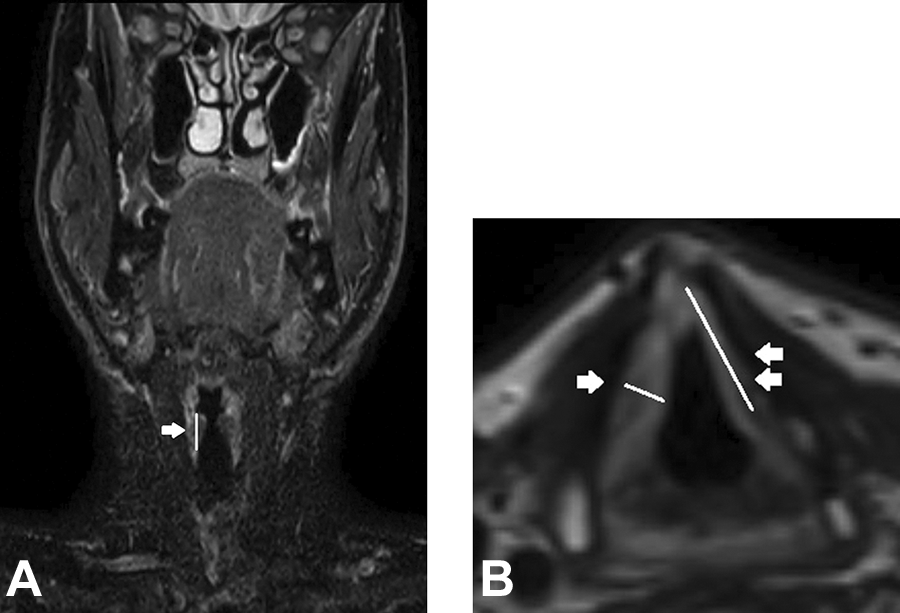
A, Coronal cut showing the height of the TA muscle as measured from its superior to inferior edge (arrow). B, Axial cut showing the length of the TA muscle as measured from the anterior commissure to the vocal process of the arytenoid cartilage (2 arrows) and its width as measured at its mid-aspect from the medial to the lateral edge (1 arrow). TA indicates thyroarytenoid.
A total of 76 patients were included (material patients of a prior investigation by the same authors on the anatomical and structural changes associated with aging). 22 Male and female groups were compared with respect to demographic data and MRI findings using parametric and nonparametric tests. 22 Independent t test was computed for normally distributed variables (age, right length, and right width) and Mann-Whitney U test was computed for the other variables. Differences were considered significant at P < .05. Further analysis was performed to investigate the association between each radiological outcome measure and gender, which was taken as a categorical variable. Statistical analysis was performed using SPSS version 23. 22
Results
Demographics
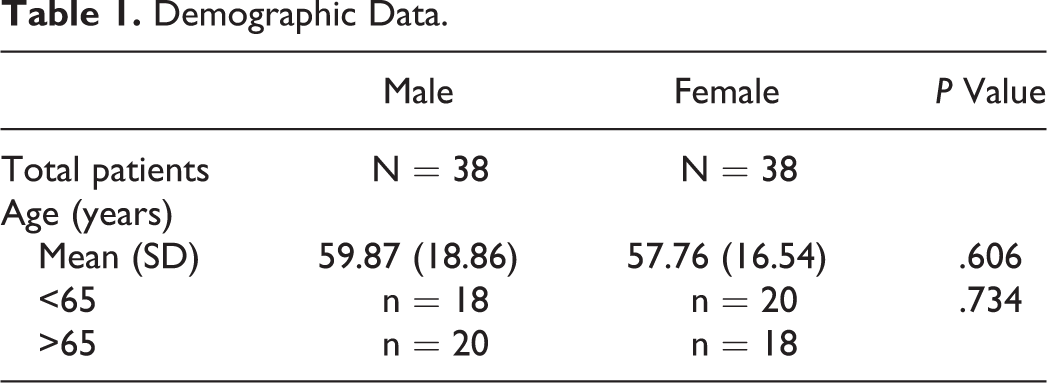
A total of 76 patients were identified and enrolled. These were divided into 38 males and 38 females. The mean age was 59.87 years in males and 57.76 years in females. The difference in mean age between both groups did not reach statistical significance (P = .606). Also, the difference between the number of patients above or below 65 years in both groups did not reach statistical significance (P = .734; see Table 1).
Demographic Data.
Magnetic Resonance Imaging Parametrical Results in the 2 Groups (Males and Females)
Length of the thyroarytenoid muscle
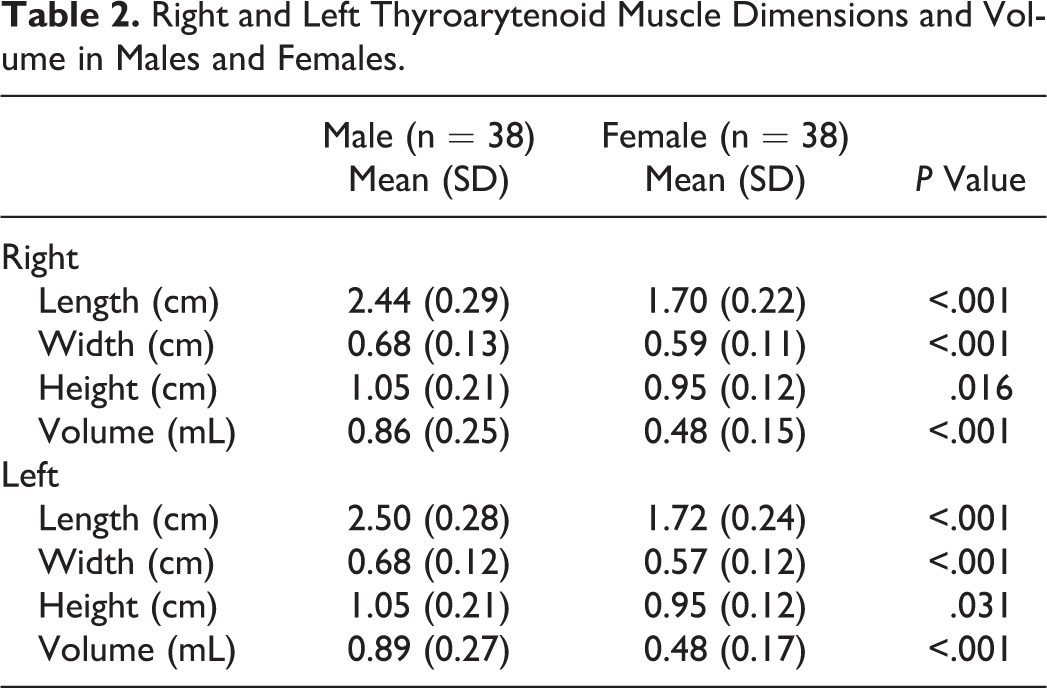
The mean length of the thyroarytenoid muscle in males was larger than that in females on the right (males 2.44 [0.29] cm vs females 1.70 [0.22] cm) and on the left (males 2.50 [0.28] cm vs females 1.72 [0.24] cm) reaching statistical significance (P < .001; see Table 2).
Right and Left Thyroarytenoid Muscle Dimensions and Volume in Males and Females.
Width of the thyroarytenoid muscle
The mean width of the thyro-arytenoid muscle in males was larger than that in females on the right (males 0.68 [0.13] cm vs females 0.59 [0.11] cm) and on the left (males 0.68 [0.12] cm vs females 0.57 [0.12] cm) reaching statistical significance (P < .001; see Table 2).
Height of the thyroarytenoid muscle
The mean height of the thyro-arytenoid muscle in males was larger than that in females on the right (males 1.05 [0.21] cm vs females 0.95 [0.12] cm) and on the left (males 1.06 [0.20] cm vs females 0.95 [0.12] cm) reaching statistical significance (P < .01 on the right and P < .05 on the left; see Table 2).
Volume of the thyroarytenoid muscle
The volume of the thyroarytenoid muscle in males was larger than that in females on the right (males 0.86 [0.25] mL vs females 0.48 [0.15] mL) and on the left (males 0.89 [0.27] mL vs females 0.48 [0.17] mL) reaching statistical significance (P < .001; see Table 2).
Discussion
Evaluation of vocal fold length in relation to the fundamental frequency using radiologic imaging dates back to several decades. Sawashima et al have reported measurements of the vocal fold length using stereoendoscope and have demonstrated the variation in the length of the vocal folds in relation to vocal registers. In their study, the vocal fold length was longer in males compared to females. 23 In 1983, Run and Chung reported the Roentgenological measurement of the physiological vocal fold length in 59 opera singers. The average vocal fold length which included the vocal process and membranous vocal fold was 21 mm (range: 16-27 mm) in males and 15 mm in females. 24 A major limitation to their study was determining the borders of soft tissue structures using plain X-ray. In another study on 100 patients undergoing direct micro-laryngoscopy, the length of the membranous vocal fold in men was reported to be 14.6 (1.2) mm and 11.1 (1.0) mm in women, with a significant difference between the 2. 25 Using computerized tomography, similar results were reported by Asahi et al. 26 The length of the membranous vocal fold was 14.8 mm and that of the total vocal fold was 25.8 mm in men. Along the same line of thought, cadaveric studies have shown a statistically significant difference in the measurements of the vocal folds among both genders. Ara et al have demonstrated in their morphometric study of the vocal folds in 29 human larynges that the mean length of the vocal fold in males was statistically higher than in females (23.12 vs 18.50 mm). 27 Similarly, the results of Mau and Courey on 23 cadaveric larynges indicated that all laryngeal measurements including vocal fold length were higher in males compared to females (15.4 vs 11.1 mm, respectively). 28
Successful extraction of 3-dimensional (3D) laryngeal measures using MRI has also enabled analysis of vocal fold vibratory behavior and vocal tract configuration during the performance of phonatory tasks in both genders. 29 Lingala et al have developed an MRI-based system for studying dynamic vocal tract shape with high-spatiotemporal resolution using a synergistic combination of custom coils, spiral acquisitions, and constrained reconstruction. 30 To that end, real-time MRI of the vocal tract during speech has become an emerging tool that provided useful dynamic information for speech research and technology development. 31 Ahmad et al investigated the vertical laryngeal movement and dynamic glottal shape using dynamic MRI. The authors reported a narrow opening during sustained vowel [i] and [u] and a large opening for [sh] in a group of 10 volunteers. 32 Markova et al demonstrated that the subjective judgment of the voice sex can be largely predicted by the morphologic and acoustic parameters in males. 33 Similarly, Vorperian et al revealed the presence of prepubertal sex differences in the oral region of the vocal tract which could explain the anatomic origin for prepubertal vowel acoustic differences among sexes. 34 Using dynamic MRI analysis, Echternach et al revealed that register transition from modal to falsetto is not primarily the result of modifications of the vocal tract whereas the use of “voix mixte” was associated with pharyngeal widening and jaw protrusion and opening. 35 In another study by the same authors, conducted on 12 professional singers the authors reported vertical rising of the larynx during pitch elevation and lowering of the larynx with an increase in loudness. 36 Similarly, Ventura et al used MRI along with 3D models to describe morphologic differences in the vocal tract cavity. The authors reported increased oral cavity volume in the singing voices and increased oral and pharyngeal cavities in the acting voices. 37
In all the aforementioned studies, the focus has been on variations in the length of the vocal folds between men and women and on the configuration of the vocal tract in relation to different vocal registers or while singing. A better understanding of the differences in vocal fold dimensions, in particular the volume of the thyroarytenoid muscle, in men compared to women, can be useful in the landscape of phonosurgery. A good example is patients with unilateral vocal fold paralysis undergoing injection laryngoplasty. The anatomical variation in the vocal fold measurements between the 2 genders mandates diligent tailoring of the site of injection as well as the amount to be injected. 28 The results of this investigation clearly corroborate the results of all the aforementioned studies on the gender differences in laryngeal dimensions. All TA measurements in the studied groups were significantly higher in males compared to females with comparable age. The most significant difference in vocal fold measurements was the length followed by the width. The difference in vocal fold height between the 2 genders was 0.55 mm comparable to the finding of Mau and Courey where the male vocal folds were 1.1 mm taller than the female vocal folds. More so the volume of the male vocal fold reported in this study was 1.81 times larger than that of the female vocal fold in comparison to the 30% to 40% difference reported by Mau and Courey. The difference in the measurements between the 2 studies can be attributed to the absence of natural tone and fixation of tissues in cadaveric studies. 28
The aforementioned gender-related differences in volumetric measures of the vocal folds not only cast further light on vocal sexual dimorphism but also carry clinical significance as previously mentioned. For instance, the difference in height of the vocal folds between the 2 genders would suggest a deeper injection in males compared to females in patients undergoing injection laryngoplasty. Similarly, the significant difference in the volume of the vocal folds in males versus females clearly translates into the need to inject more in a male patient presenting with unilateral vocal fold paralysis compared to a female patient with the same condition as reported by Mau and Courey who advise a 50% more material for injection in males. 28
This study is the first magnetic resonance study that examines the volumetric measures of the thyroarytenoid muscles in relation to gender. However, its main limitation is the lack of endoscopic images and acoustic parameters to correlate with the radiologic findings. Another limitation is the 4-mm MRI slice thickness which is not designed for the assessment of small muscles such as the thyroarytenoid muscle. Future investigations on the predictive and prognostic value of these radiologic measures in patients undergoing injection laryngoplasty will be conducted.
Conclusion
Radiological reports on volumetric measurements of the vocal fold are rare. The results of this investigation clearly indicate a significant difference in these measurements between men and women. Studying the volumetric measurement differences between genders is crucial to understanding voice sexual dimorphism and its clinical correlate in injection laryngoplasty.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.