
Abstract

The tenosynovial giant cell tumor (TGCT) is a rare, benign neoplastic process which arises from synovial cells of the joints. Tenosynovial giant cell tumor exists in either localized or diffuse form. The localized form is more frequent and appears in the smaller joints of the extremities. In contrast, the diffuse pattern is less common and usually affects the larger joints such as the hips and knees. 1 Although TGCT is a benign neoplasm, it is often locally destructive with resultant functional and cosmetic deficits. 2,3 Tenosynovial giant cell tumor has rarely been described in the temporomandibular joint (TMJ). 2 -4 In this region, it can be locally aggressive and has potential to invade the adjacent temporal bone, the skull base, and the external auditory canal. Patients typically presents with painless swelling, ear fullness, and trismus. Histopathology reveals mononuclear cells interspersed with mononuclear giant cells. 5,6 The treatment is complete surgical resection and the recurrence rate is low.
A 42-year-old male presented with few months history of left ear fullness associated with subjective hearing loss and “crunching” noise when eating. Ear examination showed a large expansile mass nearly occluding the ear canal. Initial biopsy of the mass revealed subepidermal collection of mononuclear and multinucleated giant cells with fibrosis and hemosiderin. The differential diagnosis at that time included TGCT versus giant cell reparative granuloma. Subsequent computed tomography (CT) and magnetic resonance (MR) imaging studies demonstrated an expansile mass involving the left ear canal, glenoid fossa of TMJ, and temporal bone with superior displacement of middle fossa dura (Figure 1). Patient underwent gross total resection of the tumor via combined transcanal and preauricular infratemporal fossa approach (Figure 2). The tumor was found to be leathery and infiltrative with extensive remodeling of temporal bone and middle fossa. Furthermore, portion of the tumor infiltrated into the ear canal, but no invasion was noted in the middle ear cavity. Histopathology confirmed TGCT (Figure 3). A 6-month surveillance CT showed no evidence of tumor recurrence.
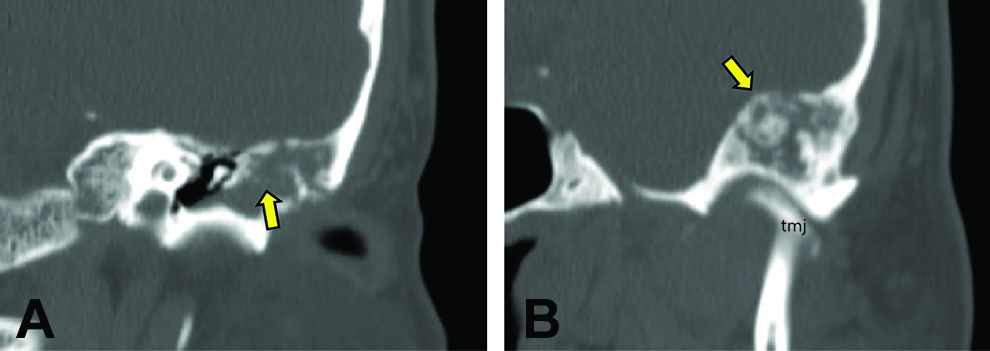
Computed tomography scan of temporal bone demonstrating TGCT with tumor infiltration into ear canal (A, arrow) and extensive remodeling of temporal bone and middle fossa (B, arrow; TMJ, temporomandibular joint). TGCT indicates tenosynovial giant cell tumor.
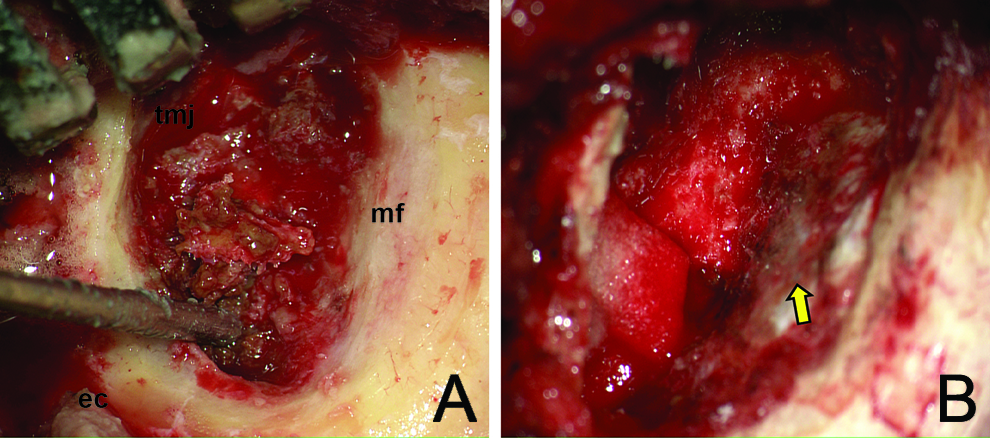
A, Intraoperative photograph showing TGCT involvement of ear canal (ec) and temporomandibular joint (TMJ) with extensive remodeling of the middle fossa (mf). B, Post-tumor resection photograph showing middle fossa dura (arrow). TGCT indicates tenosynovial giant cell tumor.
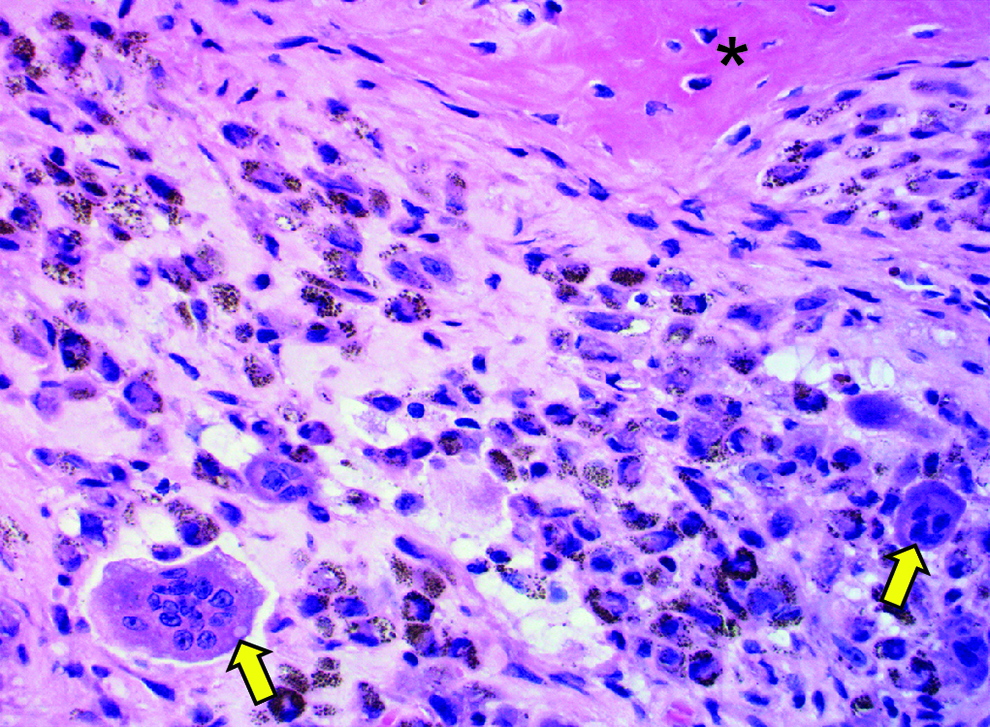
A, High magnification (×400) showing giant cells which are unique to this tumor (yellow arrows); bone is also shown (asterisk).
Tenosynovial giant cell tumor occurs with nearly equal frequency in males and females. It is a locally expansile neoplasm with varying degrees of involvement of the middle ear, external auditory canal, temporal bone, and zygomatic arch. It rarely extends to the otic capsule; however, intracranial extension was present in 33% of the cases. 2,7 The most common clinical presentations are ear fullness, pain, a preauricular mass, and trismus. In addition, hearing loss, tinnitus, and vertigo are not uncommon presenting symptoms. Biopsy of the mass is feasible in most circumstances and will show mononuclear synovial-type cells with hemosiderin-laden cytoplasm, with frequent multinucleated giant cells. Diagnostic workup should include CT and/or MR of the temporal bone, which typically shows an expansile lesion of the glenoid fossa, with varying degree of temporal bone erosion.
The primary treatment modality for TGCT is surgery. Potential surgical complications include a temporary facial nerve paresis, temporary malocclusion as well as sensorineural hearing loss in cases where the otic capsule is involved by the tumor. 2,3 The recurrence rate following surgery varied from 15% to 29% depending on the length of follow-up. 8 Therefore, a long-term clinical and radiographical surveillance is necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.