
Abstract
A 26-year-old nonsmoker male patient presented to emergency department with the complaint of severe sharp throat pain he experienced while he was eating hamburger. Further questioning revealed that he had been cleaning his grill with a wire bristle brush prior to cooking. He denied shortness of breath, hoarseness, or hemoptysis. A soft tissue neck X-ray revealed what appeared to be a wire bristle in the base of the tongue. He was transferred to a larger community hospital, where the flexible laryngoscopy suggested the tip of a small wire protruding from the tongue base which was difficult to visualize. The Ear, Nose and Throat (ENT) surgeon recommended laryngoscopy under general anesthesia for removal of foreign body. In operation room (OR), after adequate anesthesia with intermittent mask ventilation, the Kleinsasser operating laryngoscope and a 0° rod lens endoscope through the laryngoscope was used, but foreign body was not visible in the tongue base. The patient was then intubated for a deliberate examination; however, neither the foreign body nor the site of entry could be visualized. Lateral fluoroscopy, anterior–posterior fluoroscopy, or bimanual examination did not help. The surgeon terminated the procedure.
Computed tomography (CT) revealed the wire was still in the tongue base (Figure 1), lying from posterior–inferior to anterior–superior. The tip of the wire was laying deep to the mucosa. The ENT surgeon contacted the author and proposed a transoral robotic surgical procedure to remove the foreign body.
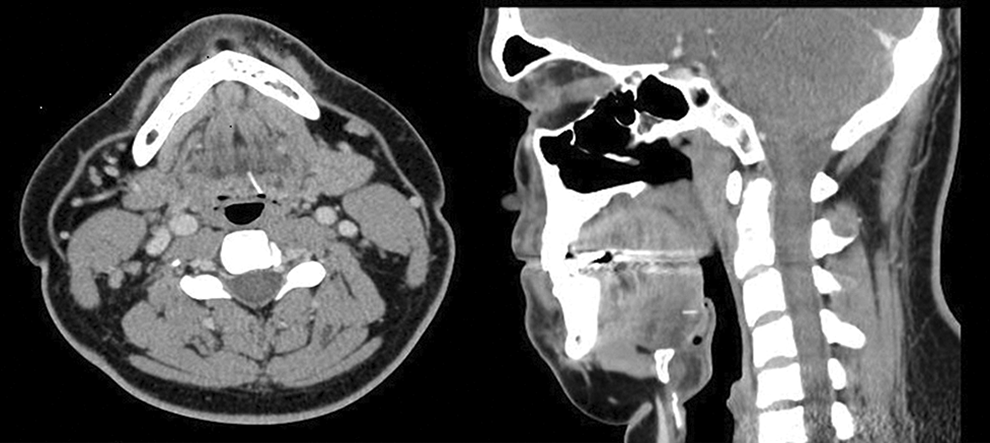
Computed tomography (CT) scan reveals wire bristle embedded in the tongue base in both axial and sagittal views.
In the referral hospital OR, after nasotracheal intubation, a self-retaining retractor was placed in the oral cavity. The left tongue base was exposed. The robot was brought into position and docked. Using a 30° scope, a mucosal flap was developed in the left base of tongue near vallecula. Dissection proceeded in the submucosal plane. A wire bristle was seen in the base of the wound (Figure 2) and was extracted using the Maryland forceps. The redundant mucosal flap was excised. Hemostasis was verified. The patient was awakened, extubated, and taken to the Post-Anesthesia Care Unit (PACU) in stable condition having tolerated the procedure well.
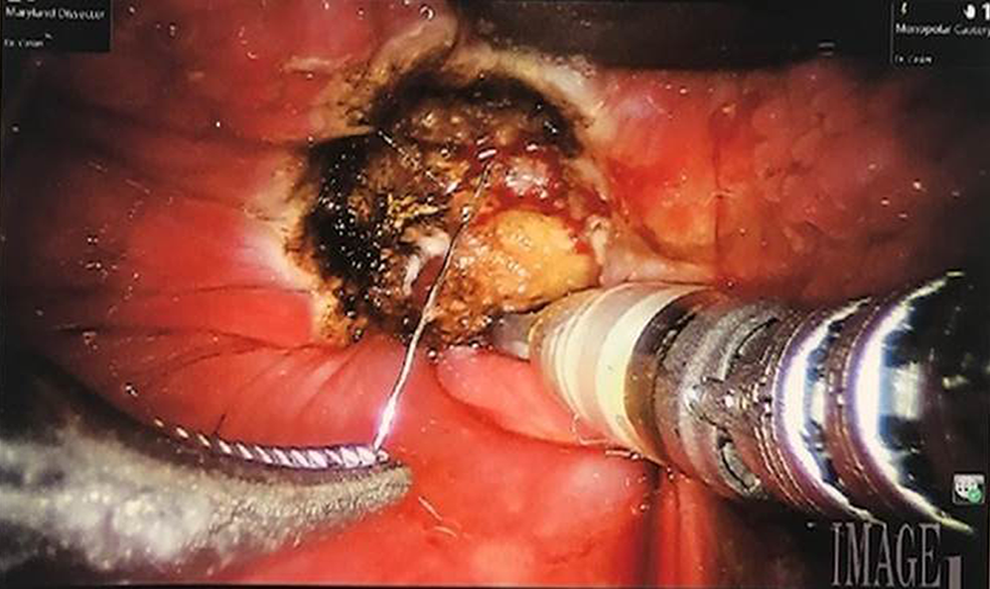
The wire bristle was seen in the base of the wound.
Discussion
Accidental wire bristle ingestion cases have been increasingly reported in recent years in both pediatric and adult population. 1 The oropharynx is the most affected location of injury after accidental ingestion. 2 Ballenger et al reported the first wire bristle ingestion case in the literature in 1952. 3 In 2012, upon receipt of increasing numbers of reported accidental wire bristle ingestion cases, The Centers for Disease Control and Prevention urged physicians, consumers, manufacturers, and retailers to be aware of the hazard and to report these cases to Consumer Product Safety Commission. 4
Considering the variety of the patient ages (10 months to 72 years) 2 and the localization that wire bristle might lodge into, colleagues in many specialties like emergency medicine, gastroenterology, surgery, and otolaryngology should be aware of these accidents and be suspicious for the correct diagnosis. A high index of suspicion during taking history is very important if endoscopic examination and plain radiograph does not reveal anything. In unnoticed cases, late removal or migration of the material might cause fatal complications which might include abscess, esophageal perforation, 5 arterial aneurysm, and carotid artery rupture. Timely and aggressive intervention is crucial to avoid these unpredictable and fatal complications.
In cases where the foreign body is seen and relatively easy to access with an angled instrument, bedside endoscopic removal can be attempted in appropriate settings. It might not be easy to localize all submucosal embedded foreign bodies endoscopically, even in the guidance of C-or O-arm fluoroscopy or CT or bimanual palpation. In specific sites like tongue base, vallecula, or deep tonsillar regions, referral to robotic surgery should always be kept in mind after unsuccessful endoscopic attempts, without waiting, in order to prevent fatal complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.