
Abstract
A 62-year-old male presented with regurgitation of food into the right nasal cavity when taking meals, especially water or liquid materials. He also complained of air flow through the mouth to the right nose. He had a history of an extraction of the right upper second molar tooth 4 months earlier and he experienced pus discharge from the extraction site 3 months after the procedure. His medical history was noncontributory. Physical examinations revealed a 3-mm-sized hole (black arrows) on the extraction site (Figure 1), and pus discharge was not noted at that time. On the paranasal sinus computed tomography, oroantral fistula was observed (white arrow) and chronic rhinosinusitis was noted in the paranasal sinuses bilaterally (Figure 2). The author postulated that preexisting chronic maxillary sinusitis and prolonged pressure due to pus collection in the right maxillary sinus caused oroantral fistula 3 months after tooth extraction. Prior to repair, bilateral endoscopic sinus surgery was performed because fistula can recur when sinus ventilation is not restored. Thereafter, the fistula was closed using the buccal mucosa and fat, and the result was successful. He is well now 6 months postoperatively and is satisfied with the result of operation.
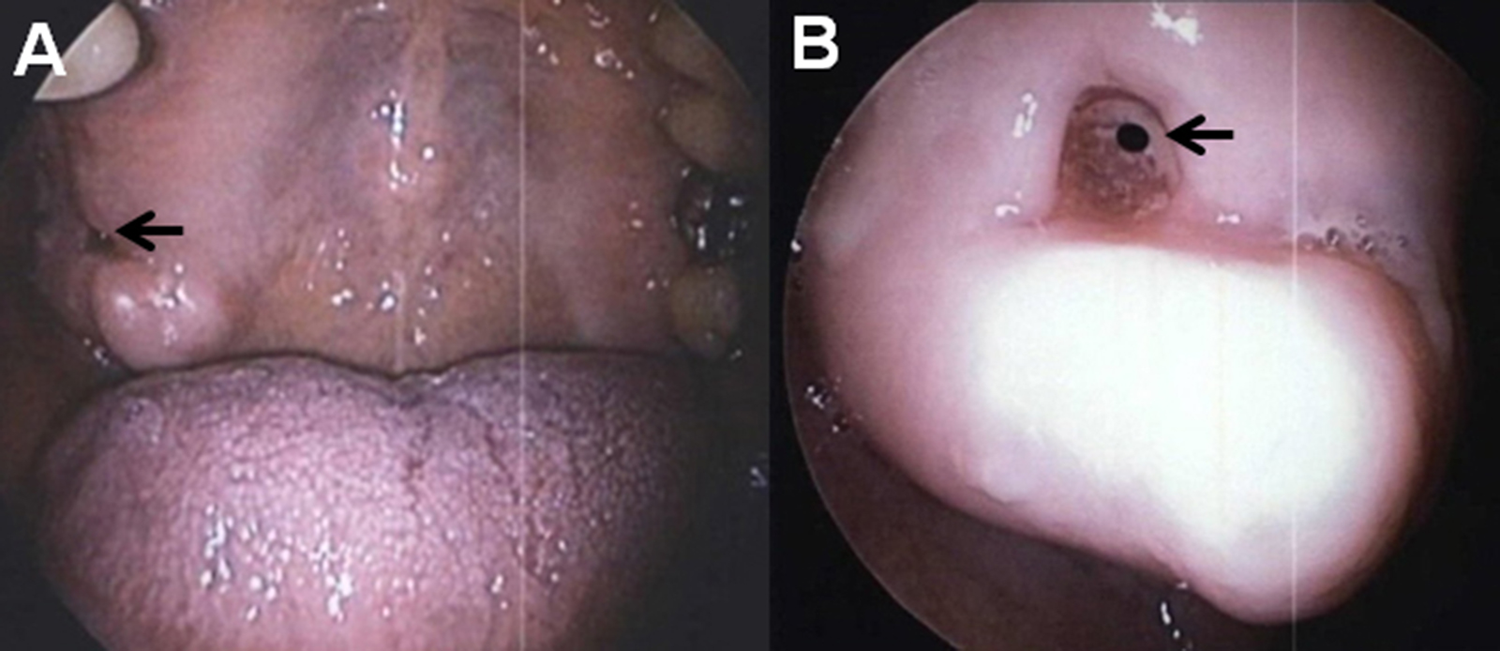
Endoscopic finding (A) shows about 3 mm sized hole on the extraction site of the right upper second molar tooth (black arrow). B, Close-up view of the oroantral fistula (black arrow).
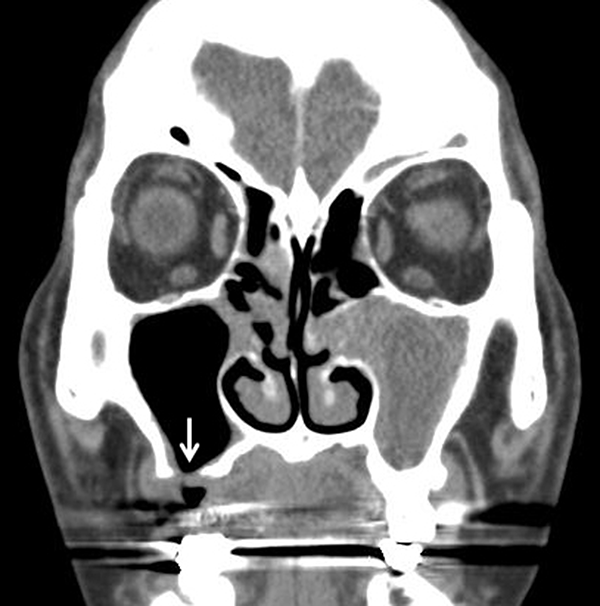
Coronal computed tomography scan shows an oroantral fistula involving the right maxillary sinus (white arrow). Chronic rhinosinusitis is noted in the paranasal sinuses bilaterally.
An oroantral communication is an open connection between the oral cavity and the maxillary sinus. It can happen due to various causes, such as the extraction of maxillary posterior teeth, implant surgery, cyst and tumor enucleation, orthognathic surgery, osteomyelitis, and trauma. 1 Many oroantral fistulas, especially those less than 3 mm in size, heal spontaneously, while those more than 3 to 5 mm in size do not heal without surgical repair. 2 Before surgical repair of the defect, elimination of the maxillary sinus pathology is essential for successful treatment.
Various surgical methods for oroantral fistula closure have been reported. The use of the buccal fat pad has increased in popularity in recent years because of its reliability, ease of harvest, and low complication rate. 3
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Soonchunhyang University Research Fund.