
Abstract

A 71-year-old female was incidentally found to have a right-sided base of tongue (BOT) mass during intubation done for a colonoscopy. The patient had a medical history of 40 years of cigarette smoking, hypertension, type II diabetes, and hypothyroidism.
Examination revealed an exophytic, lobulated right BOT mass. No neck masses were palpated. Magnetic resonance imaging of the neck demonstrated a right BOT mass measures approximately 11 mm × 16 mm × 18 mm (Figure 1) and prominent right level 2 lymph nodes.
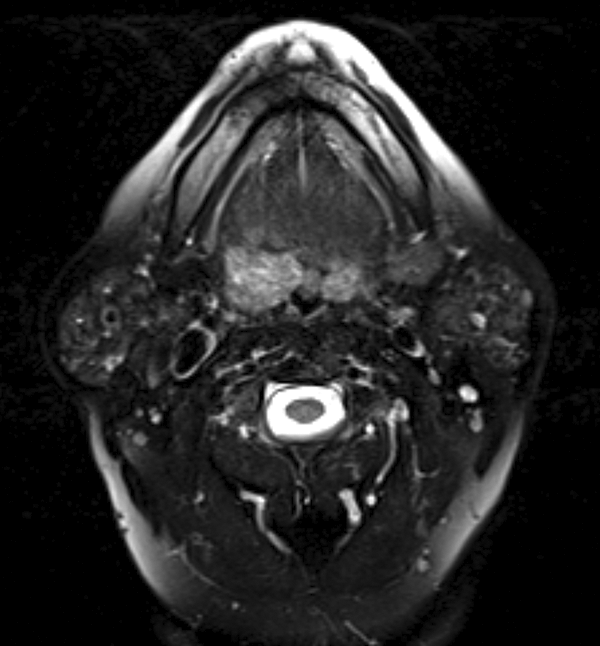
Axial neck MRI T2 image with fat saturation demonstrates 11 mm × 16 mm × 18 mm base of tongue mass. MRI indicates magnetic resonance imaging.
The patient underwent transoral robotic assisted right BOT biopsy. Histopathology revealed hyalinizing clear cell carcinoma (HCCC) of the minor salivary gland origin.
Positron emission tomography-computed tomography demonstrated fluorodeoxyglucose avidity of the right BOT and right level 2 lymph nodes (Figure 2).
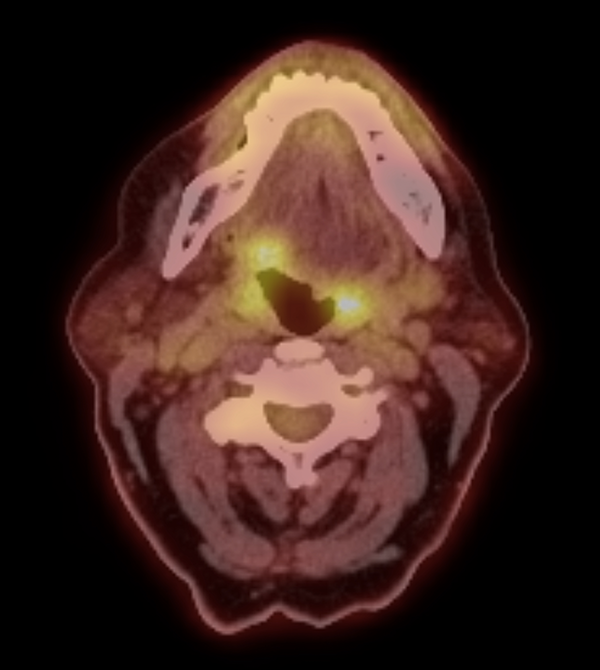
Axial fluorine 18 fluorodeoxyglucose (FDG) positron emission tomography demonstrates abnormal FDG avidity in right base of tongue mass. (Physiological FDG avidity is present in the palatine tonsils.)
The patient was subsequentially referred for definitive chemoradiation therapy. Hyalinizing clear cell carcinoma is a rare salivary gland tumor with myxoid or hyaline degeneration of the stroma arranged in trabeculae, nests, and cords that more commonly originated in the female genital tract. 1 Hyalinizing clear cell carcinoma can appear in all salivary gland sites with squamous differentiation but mostly presents in the oral cavity at the base of the tongue, palate, or parotid glands with the potential to metastasize to locoregional lymph nodes. 1,2 Clear cell carcinomas account for only 1% to 2% of all primary salivary gland tumors. 3 Women in their sixth or seventh decade of life are more affected than men. 4
Differentiating HCCC from other salivary gland clear cell tumors, such as mucoepidermoid carcinoma (MEC), epithelial
Hyalinizing clear cell carcinoma is typically low grade and not associated with a significant disease-related mortality; however, there are documented high-grade cases, for which metastatic regional lymph node assessment is recommended. 9,10 Treatment includes primary surgical resection followed by radiation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.