
Abstract
The objective of this study was to compare the effect of curative 3-dimensional (3D) conformal radio-chemotherapy and intensity-modulated radiotherapy (IMRT) modalities on swallowing function in patients with nasopharyngeal cancer. Ten patients receiving 3D conformal radiotherapy and 10 patients receiving curative radiotherapy with IMRT, who were admitted for malignancy control for nasopharyngeal cancer, were included in the study. Swallowing functions were determined by flexible fiberoptic endoscopic evaluation. Premature spillage, retention pooling, penetration, aspiration, and reflex cough were evaluated. No statistically significant difference was found between patients receiving 3D conformal radiotherapy and IMRT regarding the scores of premature spillage, retention pooling, penetration, and aspiration with 3, 5, and 10 mL water and 5 mL yoghurt and fish crackers (P > .05). Velopharyngeal insufficiency or delayed onset of swallowing reflex was not found in any of the patients (P > .05). No significant difference was found between the groups in terms of the symptoms regarding subjective evaluation of swallowing (P > .05). Swallowing function did not differ among patients receiving IMRT and 3D conformal radiotherapy. Further studies with a larger sample size are warranted in order to verify the results.
Keywords
Introduction
Improvements in early diagnosis and treatment modalities of nasopharyngeal carcinoma have provided significant improvement in the survival rate and quality-of-life parameters. 1 Radiotherapy is the main treatment modality in nasopharyngeal cancer without an alternative, except for the rare histological types such as adenocarcinoma that require surgery. 2,3
Currently, the most common types of radiotherapy include conformal therapy and intensity-modulated radiotherapy (IMRT), where the intensity of beams radiating from the device can be modulated. IMRT is important for the small-segment irradiation that enables the protection of surrounding tissues while administering higher dosages to the target. 4 -8 However, various early and delayed side effects might still be observed following radiotherapy, despite advances in radiotherapy techniques. These late effects include dysphagia, mucositis, xerostomia, impaired taste perception, dental caries, trismus, and cranial nerve palsies. 2,3
Side effects influencing the quality of life gradually gained more importance with the increase in survival rates. Dysphagia is among these side effects influencing the quality of life. Decreased pharyngeal motility, increased pharyngeal residue, epiglottal immobility, closure defect of the laryngeal vestibule, and aspiration have been reported in patients with nasopharyngeal cancer receiving radiotherapy. 9 -14 There are studies suggesting fewer adverse effects on swallowing functions with the IMRT technique due to its technical advantages and clinical results. 15,16 However, a study using fiberoptic endoscopy to demonstrate the superiority of IMRT to 3-dimensional (3D) conformal therapy in terms of swallowing function in patients with nasopharyngeal cancer does not exist. The objective of this study was to compare the effects of curative 3D conformal radiotherapy and IMRT on swallowing function in patients with nasopharyngeal cancer.
Materials and Methods
Twenty-eight patients with nasopharyngeal cancer who were referred to the radiation oncology clinic of a tertiary academic center between January and June 2013 and met the study inclusion criteria were included in this study. Informed consent was obtained from all the patients. This study was approved by the institutional review board.
Eight patients were excluded from the study: 5 patients for not attending their scheduled visits, 2 patients for refusing to participate in the study, and 1 patient for having distant metastasis. Ten patients were recruited in the 3D conformal radiotherapy group, and 10 patients were recruited in the curative radiotherapy with IMRT group. All the patients were treated with concurrent chemotherapy. Patients were randomly assigned to one of the groups.
Study inclusion criteria were as follows: being 20 to 60 years old, history of prior radiotherapy or chemotherapy, absence of residual tumor or distant metastasis, symptoms of any spectrum of dysphagia, willingness to participate in the study, and the cognitive capability to comprehend and follow the study directives. Study exclusion criteria were cranial nerve involvement, history of surgical therapy, and tumor recurrence during the study.
There were 3 (30%) females and 7 (70%) males in the 3D conformal therapy group and 2 (20%) females and 8 (80%) males in the IMRT group. Mean age was 43.10 (±13.62) years and 43.80 (±11.32) years in the IMRT and 3D conformal radiotherapy groups, respectively. Patients received 33 or 35 radiotherapy courses and 3 to 7 chemotherapy courses. Radiotherapy was administered at 60 to 70 Gy depending on the nasopharyngeal spread; 70 Gy was administered to the lymph nodes, and 66 Gy was administered to the remaining neck tissue in patients with positive neck lymph nodes. The entire neck region was irradiated with 66 Gy in patients without jugular lymph node positivity.
Procedure
Sociodemographic data were obtained from medical records and via interview prior to any study procedure. Parameters including the diagnosis, number and method of radio-chemotherapy courses, pathology, and duration passed after the radio-chemotherapy were recorded in case evaluation forms. Additionally, certain types of foods triggering the dysphagia, any difficulties in bolus control, the need to clean the throat, sensation of having a lump in the throat, and sensation of choking, cough, and xerostomia were questioned. Endoscopic examination was performed to evaluate velopharyngeal insufficiency, movements of vocal cords, and any delay in the onset of swallowing, and a physical examination was performed to evaluate movements of the tongue and soft palate.
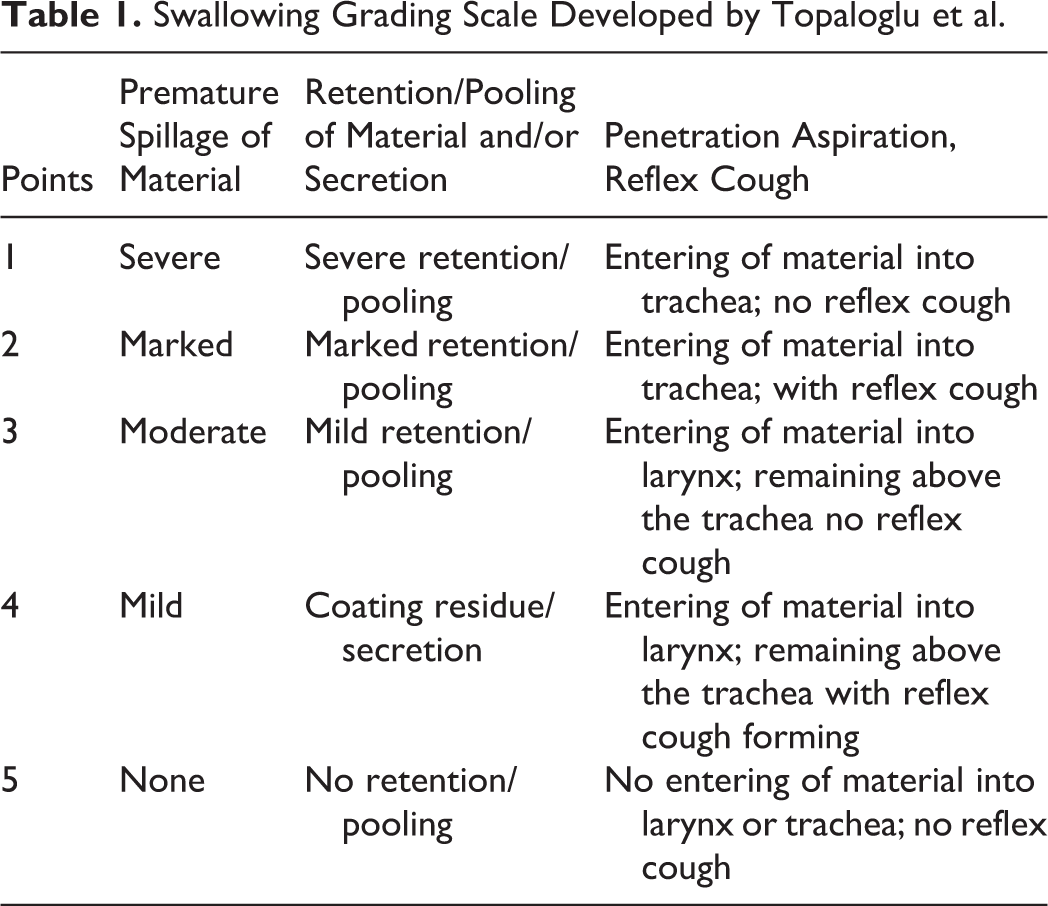
Intravenous access was secured, and a pulse oximeter was connected to each patient prior to the procedures. Next, video fiberoptic endoscopy was administered in an upright seated position without administering topical anesthesia to the nasal cavity, and video recordings were obtained in each patient (Kay Pentax Ltd, Montvale, New Jersey). A flexible nasopharyngoscope camera (3.6 mm diameter; Olympus, Tokyo, Japan) was used during the procedures. Any velopharyngeal insufficiency in the nasopharyngeal region against solid, liquid, or semi-liquid foods was evaluated. Next, the laryngopharynx was observed to determine the movements of the vocal cords during respiration and phonation. The test protocol included 2 administrations of 3, 5, and 10 mL of water colored with food dye (green) via an injector. Similarly, swallowing tests were performed with 2 administrations of 1 dessert spoonful of yoghurt (5 mL) colored with food dye and fish crackers. Premature spillage, retention pooling, penetration, aspiration, and reflex cough were scored (from 1 to 5) using the scoring system of Topaloglu et al (Table 1). 17 An otolaryngologist and a physical therapy and rehabilitation specialist were present during each procedure, and all procedures were video recorded. Endoscopic examination was performed 6 months after the last irradiation dose. All test results were assessed by the same physician specialized and experienced in this area and the same otolaryngologist in a blinded manner independent of the treatment protocols.
Swallowing Grading Scale Developed by Topaloglu et al.
Statistical Analysis
Statistical analysis was made using computer software (SPSS version 17.0, SPSS Inc, Chicago, Illinois). A P < .05 was considered statistically significant. Nonparametric tests were performed since the data did not have normal distribution. χ2 analyses and Mann-Whitney U tests were performed in discontinuous variables. Descriptive statistics were performed for demographic data. All results were presented as mean (standard deviation).
Results
There was no significant difference between the 2 groups in terms of sociodemographic features (P > .05). The histopathological diagnosis was undifferentiated carcinoma in 8 (80%) patients, nonkeratinized squamous cell carcinoma in 1 (10%) patient, and keratinized squamous cell carcinoma in 1 (10%) patient in the 3D conformal radiotherapy group, whereas the histopathological diagnosis was undifferentiated carcinoma in 9 (90%) patients and non-keratinized squamous cell carcinoma in 1 (10%) patient in the IMRT group. The stages of the 10 patients in the 3D conformal radiotherapy group were stage 3 in 7 patients, stage 2 in 2 patients, and stage 1 in 1 patient. The stages of the 10 patients in the IMRT group were stage 3 in 5 patients and stage 2 in 5 patients. The relation between the stage of the disease and the RT method was statistically insignificant (P > .05; Table 2).
The Relation Between the Stage of the Disease and Radiotherapy Modalities.
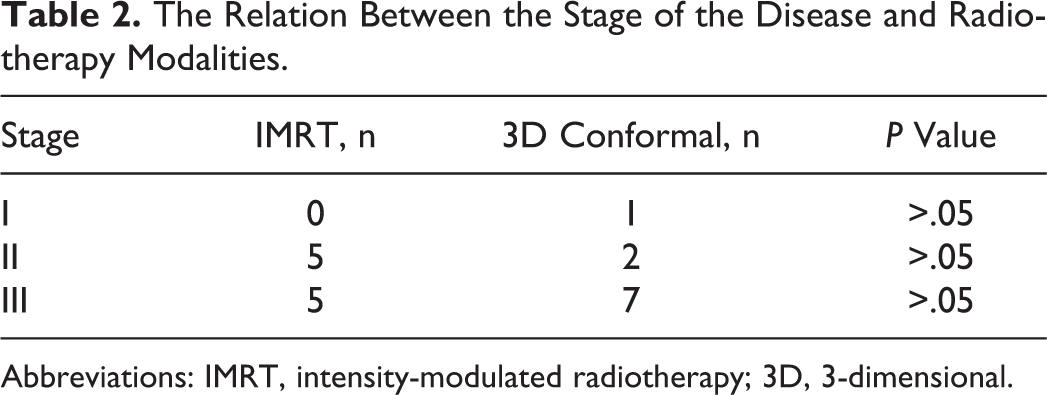
Abbreviations: IMRT, intensity-modulated radiotherapy; 3D, 3-dimensional.
No significant difference was found in the scores of premature spillage, retention pooling, penetration, and aspiration with 3, 5, and 10 mL water, yoghurt, and fish crackers in patients with nasopharyngeal cancer receiving 3D conformal radiotherapy and IMRT (P > .05; Table 3).
Evaluation of Dysphagia Parameter in Patients With Nasopharyngeal Cancer Receiving 3D Conformal Radiotherapy and IMRT With 3, 5, and 10 mL Water, Yoghurt, and Fish Crackers.
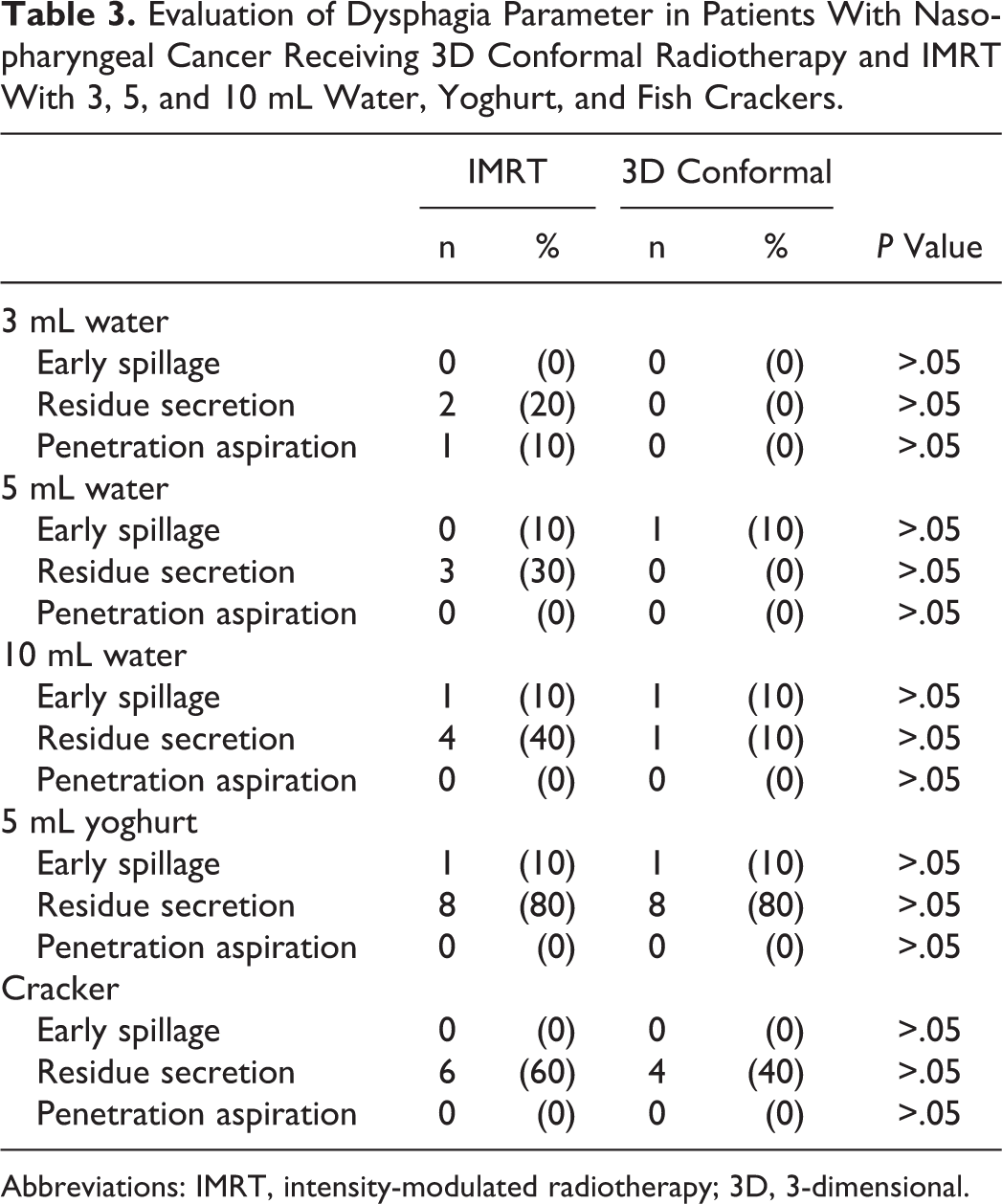
Abbreviations: IMRT, intensity-modulated radiotherapy; 3D, 3-dimensional.
Xerostomia and desire to take solid food with water was assessed in all the patients in both the groups (100%). No significant difference was found between the 2 groups (P > .05). Movements of the vocal cords and tongue were normal in all patients. Velopharyngeal insufficiency and delayed onset of swallowing were not found statistically different in any of the patients (P > .05; Table 4). Rates of the symptoms regarding subjective evaluation of swallowing did not differ significantly between the groups, and the data are presented in Table 4 (P > .05).
Rates of Symptoms Regarding Subjective Evaluation of Swallowing in Patients With Nasopharyngeal Cancer Receiving 3D Conformal Radiotherapy and IMRT.
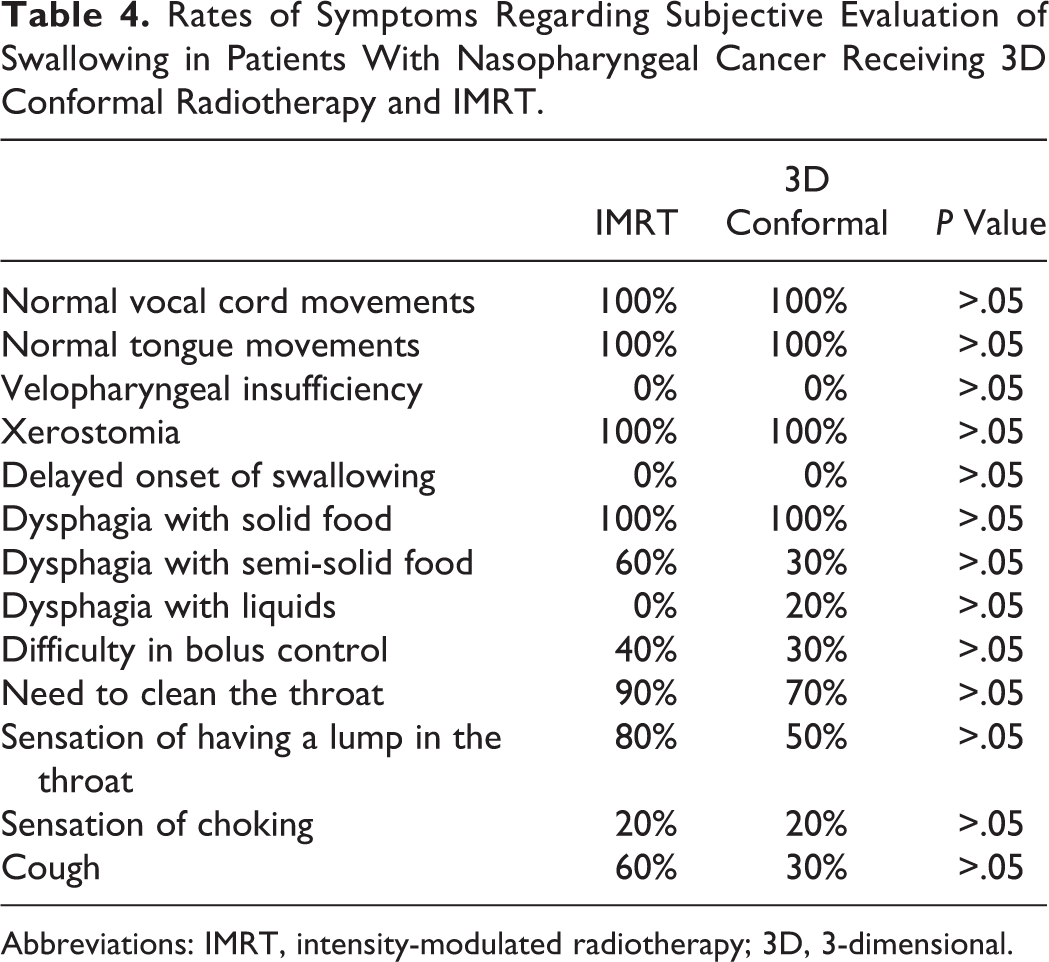
Abbreviations: IMRT, intensity-modulated radiotherapy; 3D, 3-dimensional.
Discussion
Swallowing function affects the quality of life significantly; therefore, approaches aimed at improving its associated symptoms have gradually gained importance. The IMRT technique has become prominent to reduce tissue and functional losses. Studies on IMRT have reported its favorable effects on swallowing functions and xerostomia. 18 -20 These favorable effects are in turn thought to affect the quality of life. In the study of Vergeer et al comparing the quality of life in patients with nasopharyngeal cancer receiving 3D conformal radiotherapy or IMRT, quality of life was reported to be higher in the IMRT group at 6 months, whereas a statistically significant difference was found in the quality of life at 3 months but not at 12 months of treatment in the similarly designed study reported by Fang et al. 21,22 Although quality of life was not assessed in this study, the hypothesis that IMRT has favorable effects on swallowing functions was evaluated.
Dysphagia is one of the late complications seen in patients receiving radiotherapy or chemotherapy for nasopharyngeal carcinoma. 2,3 The effect of the specific RT modality on swallowing functions has been a question of interest. Certainly, xerostomia also has significant negative effects on swallowing.
The most common complaint was xerostomia (100%) and associated dysphagia with solid foods in both the groups. No statistically significant difference was found between the patients in IMRT and 3D conformal therapy groups. Several studies have reported reduced irradiation of the parotid gland with IMRT and therefore reduced impairment of saliva secretion with this modality compared to conformal therapy. 19,20 Similar to this study, other studies have reported lymph node metastasis in 85% of the patients, making the avoidance of the parotid gland form neck radiotherapy impossible. 23,24 Therefore, it is difficult to suggest that IMRT has more favorable effects on xerostomia by the current and other previous data.
Premature spillage, penetration, and aspiration were uncommon in both the groups; however, residue in the form of coating was common with yoghurt and crackers. The most common problem associated with swallowing was reported as coating in the videofluoroscopic study of Chang et al. 25 Reduced saliva secretion secondary to radiotherapy was reported to cause coating in the study of Kapila et al. 26 Wu et al performed a fiberoptic endoscopic study and reported pharyngeal residue (93.5%) as the most common problem that was associated with post-swallowing aspiration. 14 No significant difference was found between the groups in this study in terms of coating. A residue of 80% was found particularly following the intake of 5 mL yoghurt in both the groups; however, no significant difference was found between the groups. These data indicate that radiotherapy modality has no significant effect on swallowing findings including residue.
Although video-fluoroscopy is the worldwide gold standard in the evaluation of swallowing, recent studies have demonstrated that fiberoptic endoscopy is also valid and reliable. Wu et al performed fiberoptic endoscopy in 31 patients with nasopharyngeal cancer and reported reduced pharyngeal contraction (93%) and laryngeal penetration and aspiration (65%). 14 Marshall et al performed videofluoroscopy in 32 patients and found laryngeal penetration (94%) and aspiration (71%) and lack of cough reflex in 87% of the patients. 27 Another study compared the fiberoptic endoscopic and videofluoroscopic evaluations of swallowing in patients with nasopharyngeal cancer and reported higher penetration aspiration scores with videofluoroscopic evaulation. 25 This has been explained with the inadequate assessment of aspiration with fiberoptic endoscopy due to pharyngeal contraction during swallowing. 25 However, aspiration during swallowing was found in all patients with vocal cord paralysis, and the importance of maintenance of normal vocal movements in protecting from aspiration has been highlighted. 26 However, greater residue, penetration, and aspiration values were found in fiberoptic endoscopic evaluation compared to videofluoroscopic assessment in the study of Kelly et al. 28 The lack of aspiration in both the groups in this study might also be explained with the normal vocal cord movements in all patients. Different radiotherapy modalities do not seem to have any effect on swallowing function in terms of aspiration and penetration.
The most powerful aspect of this study is being the first study to evaluate and compare swallowing functions using fiberoptic endoscopy in patients with nasopharyngeal cancer receiving conformal radio-chemotherapy and IMRT. Results have been obtained in a blinded manner with objective evaluation methods rather than questioning by a specialist or survey administration. However, the study limitations were the low number of patients, lack of randomized controlled grouping prior to treatment, and the absence of quality-of-life questionnaires. Additionally, xerostomia was investigated subjectively by patient questioning. Therefore, it should be noted that xerostomia evaluation was not objective.
Conclusion
Swallowing function was compared in patients with nasopharyngeal cancer receiving IMRT or 3D conformal radiotherapy, and no significant difference was found between the groups. These results and the related previous data suggest that radiotherapy modalities do not differ in terms of their side effects on swallowing functions. Therefore, further studies are warranted with greater number of patients to verify these results.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.