
Abstract

A 20-year-old female with a past medical history of asthma, anxiety, and depression presented multiple times to a tertiary care center for recurrent episodes of tongue swelling, pain, and respiratory distress. She reported that these episodes started when she was an infant, when she had a procedure done in her home country of Mexico to treat an enlarged tongue. Since then, she had had several admissions to the medical intensive care unit at a tertiary care center for treatment of idiopathic tongue swelling presumed to be angioedema. Physical examination findings were significant for a grossly enlarged, tender tongue with red vesicles diffusely present on the anterior two-thirds dorsal and ventral surfaces (Figure 1).
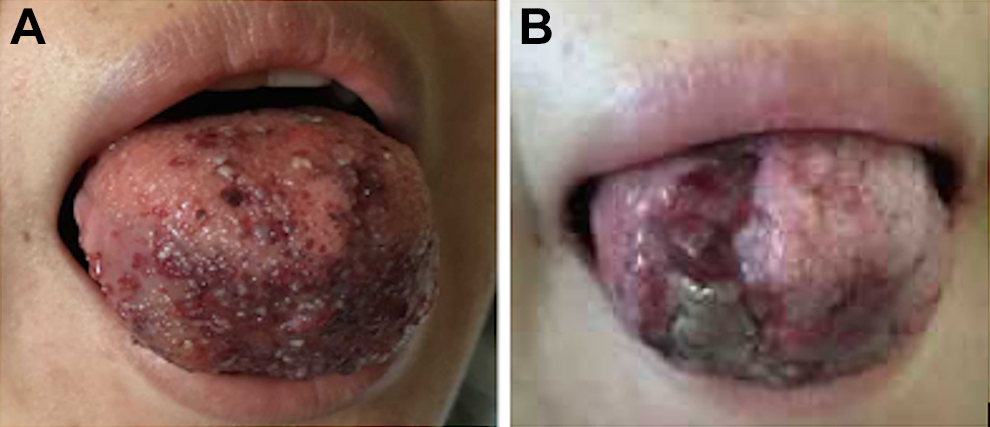
Left: physical examination reveals a grossly enlarged, edematous tongue that is firm to palpation. There are also multiple scattered red vesicles present on the anterior two-thirds of the dorsal and ventral surfaces of the oral tongue. Right: Photograph taken 2 weeks after embolization reveals areas of necrosis and gross shrinkage of overall tongue volume.
She improved clinically each time with the administration of steroids, antihistamines, and epinephrine. She had multiple imaging studies—including magnetic resonance imaging (MRI), magnetic resonance angiography (MRA), ultrasound, and computed tomography (CT)—all of which revealed an enlarged tongue but with no discrete mass or vascular anomaly (Figure 2). She also had extensive rheumatologic and infectious workup without a definitive diagnosis.
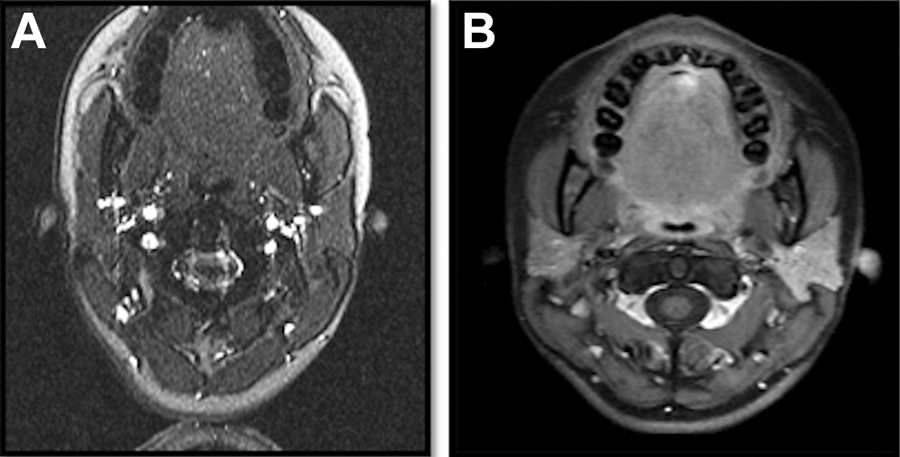
Imaging studies including axial images through the patient’s tongue—MRA (left) and nonenhanced T1-weighted MRI (right)—show no gross abnormality of the tongue, including the absence of any vascular malformation. MRA indicates magnetic resonance angiography; MRI, magnetic resonance imaging.
She eventually underwent a punch biopsy of the tongue. Histopathology showed vascular proliferation with a predominant lymphangiomatous component, supporting the diagnosis of lymphatic malformation (LM). She ultimately underwent embolization of the tongue, which to date has shown significant improvement in her tongue swelling episodes.
Errors in vasculogenesis are broadly classified as either vascular tumors (hemangiomas) or vascular malformations (venous malformations, arteriovenous malformations, LMs, capillary malformations, and mixed) based on vessel architecture. 1 In hemangiomas, blood vessel architecture is incomplete and surrounded by rapidly dividing endothelial cells. In vascular malformations, there are enlarging ectatic vessels composed of a particular architecture of veins, lymphatic vessels, venules, capillaries, arteries, or mixed vessel types. 2
Lymphatic malformations are the second most common type of vascular malformation after venous malformations. More than 90% of all LMs occur in the head and neck, including the cheek, tongue, and floor of mouth. 3 Diagnosis is usually made at birth or during childhood when the lesions become apparent during acute infections such as upper respiratory tract infections or otitis media. These infections can cause swelling of the malformation due to increased lymphatic flow. Common presenting complaints include obvious facial deformity, pain, airway obstruction, odynophagia, dysphagia, speech difficulty, and infection of the malformation itself. 2 Diagnosis usually begins with a high clinical suspicion followed by imaging studies.
Ultrasound is often the preferred initial imaging test as it is the least invasive and can be easily carried out in the outpatient clinic, but it cannot always demonstrate the deep component of the lesion accurately. Magnetic resonance imaging/MRA is often cited as the modality of choice because of its superior soft tissue resolution. Lymphatic malformations typically appear with high signal intensity on T2-weighted imaging due to its high water content and may demonstrate some layering within cystic components. 4 Computed tomography is limited in assessing vascular anomalies but can be useful for assessing bony involvement and in detecting intralesional phleboliths. 4
The current case demonstrates, however, that imaging modalities may not always be reliable in obtaining a diagnosis of vascular malformations. Our particular patient underwent all of these imaging studies, but because the correct diagnosis was not obtained, she was repeatedly treated for angioedema with temporary resolution of her symptoms.
In the current literature, there are only a handful of cases described of LMs of the tongue. Yesil et al describe the case of a 1-year-old girl with macroglossia and feeding difficulties, whose MRI revealed a “heterogeneous hypervascular solid/cystic mass with unclear borders” that involved the anterior two-third of the tongue. 5 Usha et al report the case of a 13-year-old girl who presented with a tongue mass and a CT angiography described low velocity of blood supply and no abnormalities of the blood vessels in the tongue. 6
It is unclear why imaging can better detect these lesions in some patients compared to others. One hypothesis may be that the current patient underwent these imaging studies during periods of acute inflammation, which may have resulted in distortion of typical LM anatomy and rendered diagnosis more difficult. Another possibility may be due to variation in radiologist technique and the difficulty of detecting a fairly rare entity especially in the mobile oral tongue.
The present case emphasizes the importance of sound clinical judgment and the pitfalls of relying solely on imaging studies. Although it is unclear why imaging may be more successful in detecting LMs in some patients compared to others, in patients with recurrent tongue swelling and an easily accessible lesion, tissue biopsy should be considered.
Footnotes
Authors’ Note
Podium presentation at Triological Society Combined Sections Meeting, New Orleans, Los Angeles, USA, on January 21, 2017.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.