
Abstract
A 78-year-old woman presented with chronic dysphonia that had worsened markedly over five months. She spoke with a strained, coarse voice with frequent phonatory breaks and reported substantial vocal fatigue and intermittent dysphagia. She was referred from a general otolaryngologist due to cystic recurrence after biopsy of a cyst of the left aryepiglottic fold that was reported as “benign.” She had no relevant past medical history except a 40 pack-year smoking history.
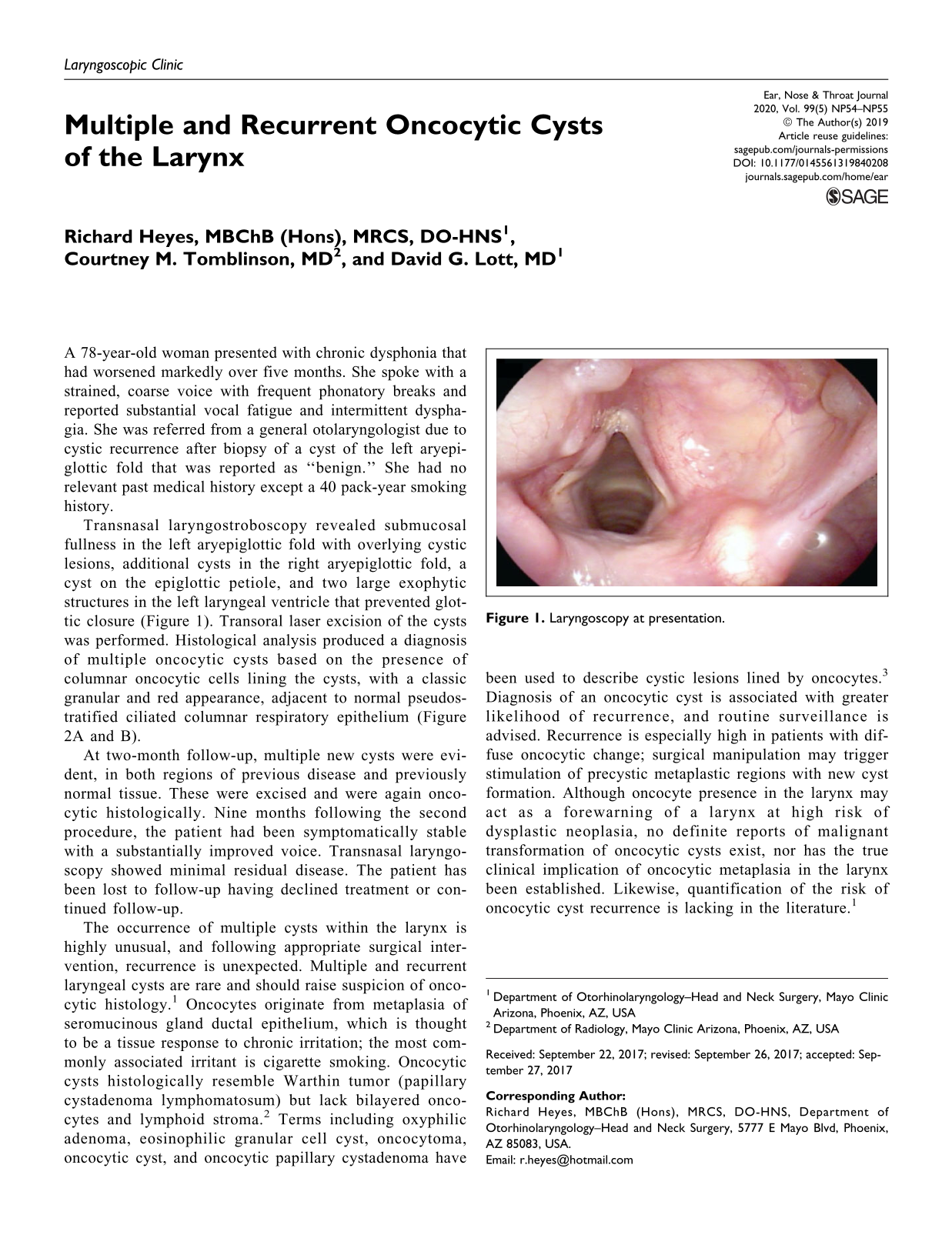
Transnasal laryngostroboscopy revealed submucosal fullness in the left aryepiglottic fold with overlying cystic lesions, additional cysts in the right aryepiglottic fold, a cyst on the epiglottic petiole, and two large exophytic structures in the left laryngeal ventricle that prevented glottic closure (Figure 1). Transoral laser excision of the cysts was performed. Histological analysis produced a diagnosis of multiple oncocytic cysts based on the presence of columnar oncocytic cells lining the cysts, with a classic granular and red appearance, adjacent to normal pseudostratified ciliated columnar respiratory epithelium (Figure 2A and B).

Laryngoscopy at presentation.
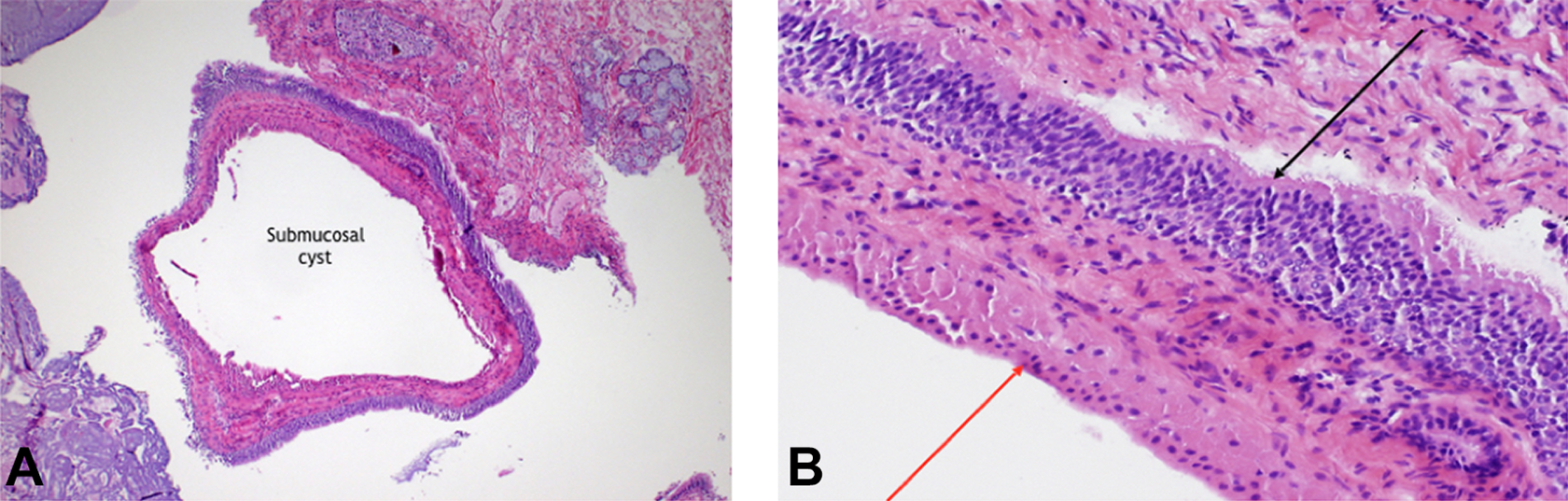
A, Left laryngeal ventricular submucosal cyst. Hematoxylin and eosin ×40. B, Cyst lining composed of columnar oncocytic epithelium (red arrow) with adjacent normal pseudostratified ciliated columnar respiratory mucosa (black arrow). Hematoxylin and eosin ×200.
At two-month follow-up, multiple new cysts were evident, in both regions of previous disease and previously normal tissue. These were excised and were again oncocytic histologically. Nine months following the second procedure, the patient had been symptomatically stable with a substantially improved voice. Transnasal laryngoscopy showed minimal residual disease. The patient has been lost to follow-up having declined treatment or continued follow-up.
The occurrence of multiple cysts within the larynx is highly unusual, and following appropriate surgical intervention, recurrence is unexpected. Multiple and recurrent laryngeal cysts are rare and should raise suspicion of oncocytic histology. 1 Oncocytes originate from metaplasia of seromucinous gland ductal epithelium, which is thought to be a tissue response to chronic irritation; the most commonly associated irritant is cigarette smoking. Oncocytic cysts histologically resemble Warthin tumor (papillary cystadenoma lymphomatosum) but lack bilayered oncocytes and lymphoid stroma. 2 Terms including oxyphilic adenoma, eosinophilic granular cell cyst, oncocytoma, oncocytic cyst, and oncocytic papillary cystadenoma have been used to describe cystic lesions lined by oncocytes. 3 Diagnosis of an oncocytic cyst is associated with greater likelihood of recurrence, and routine surveillance is advised. Recurrence is especially high in patients with diffuse oncocytic change; surgical manipulation may trigger stimulation of precystic metaplastic regions with new cyst formation. Although oncocyte presence in the larynx may act as a forewarning of a larynx at high risk of dysplastic neoplasia, no definite reports of malignant transformation of oncocytic cysts exist, nor has the true clinical implication of oncocytic metaplasia in the larynx been established. Likewise, quantification of the risk of oncocytic cyst recurrence is lacking in the literature. 1
Footnotes
Authors’ Note
This case was presented at The Triological Society’s Combined Sections Meeting in Scottsdale; January 24-26, 2013; Arizona. This case report was deemed IRB exempt.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.