
Abstract
Congenital laryngeal cysts were described first by Abercrombie in 1881 1 and present a life-threatening condition which can compromise the upper airway. Congenital laryngeal cysts are rare with an incidence of 1.82 per 100 000 live births, 2 and urgent surgical intervention is considered the mainstay intervention. 3
A 3-day-old term baby had been referred to our service with mild intermittent inspiratory stridor and a hoarse cry that had been present since birth. No significant family history was noted. The baby did not require respiratory support, was not desaturating on room air, and had established breastfeeding. Prenatally, fetal ultrasound scans detected both renal and hepatic cystic lesions.
A decision was made to assess the airway in the operating room under general anesthesia with laryngobronchoscopy and potentially transoral endoscopic marsupialization of a cyst. Laryngobronchoscopy was performed under general anesthesia with spontaneous ventilation, and a large saccular cyst was diagnosed. The cyst involved the right aryepiglottic fold with compression of the right vocal fold and some airway compromise (Figures 1 and 2). No secondary airway pathology was noted down to the level of the bronchi. Transoral endoscopic cyst marsupialization was performed using cold instruments. Following this procedure, the lateral compression against the right vocal fold was completely reduced. The baby was transferred back to neonatal intensive care unit and her stridor and hoarseness had resolved. Follow-up direct laryngoscopy in the operating room 2 weeks later showed complete resolution (Figure 3). Histology sections showed findings consistent with a simple cyst. The baby was diagnosed further with cystic biliary atresia and polycystic kidney disease. Detailed chromosome test (microarray) did not detect any clinically significant imbalance. A multidisciplinary meeting including the neonatology team, clinical genetics, and gastroenterology took place, and the shared decision was that the clinical presentation is consistent with a ciliopathy.
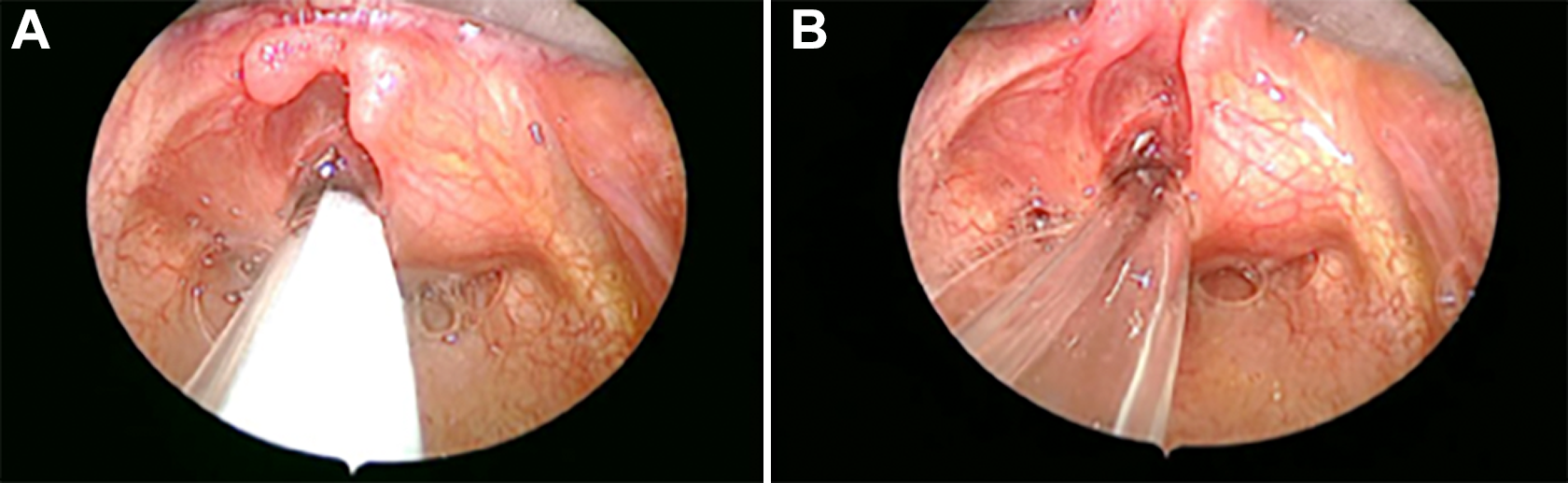
Saccular cyst prior to removal (A and B).
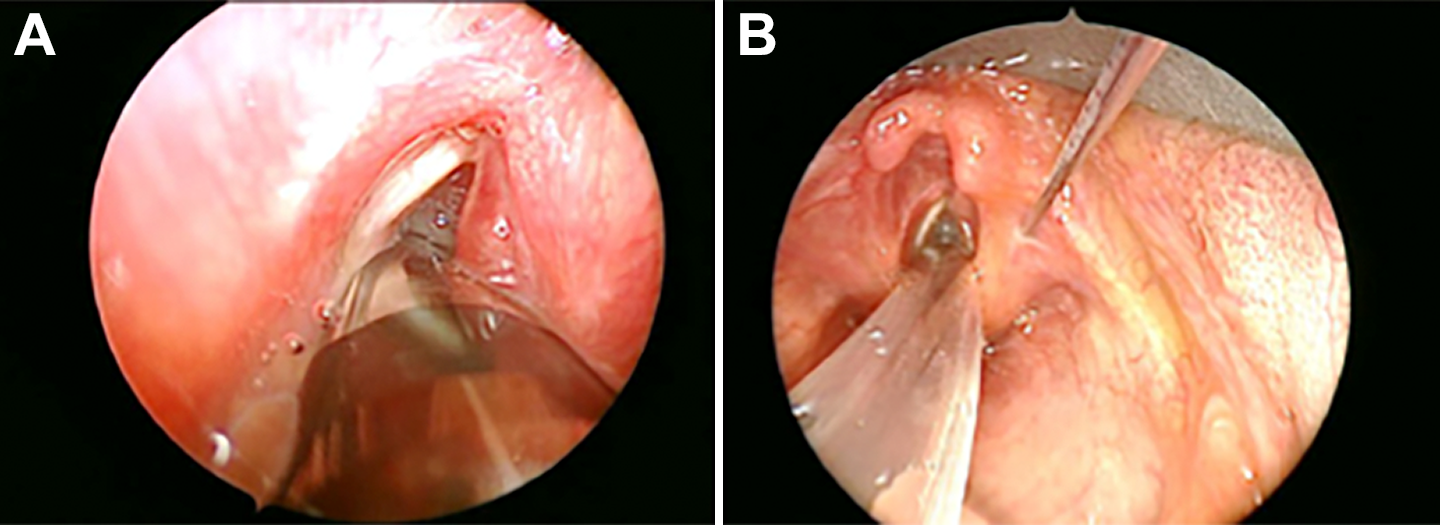
Cyst compressing against right vocal cord (A) and a needle inside cyst (B).
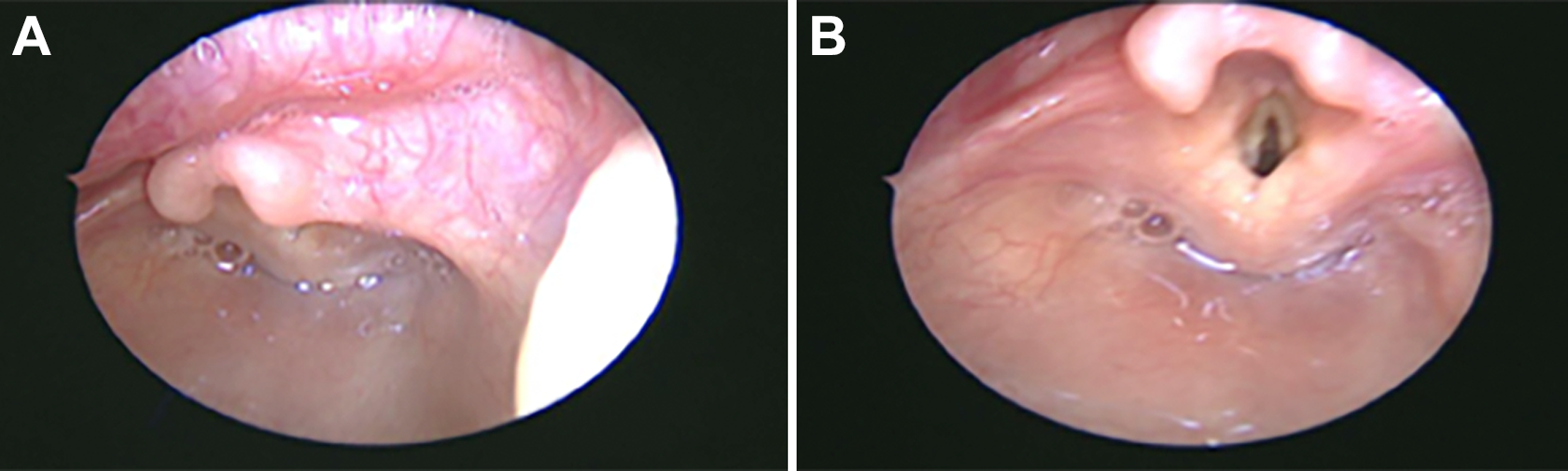
Follow-up 4 weeks after marsupialization. Right lateral view (A) and medial view (B).
This case suggests potential laryngeal cyst involvement in babies with ciliopathies. Ciliopathies present as a group of disorders associated with genetic mutations encoding faulty proteins, which result in either abnormal formation or function of cilia. 4
Difficult to determine whether there was a causal relationship between the presence of a saccular cyst and ciliopathy and these may have been coincidental. Congenital laryngeal cysts may cause an unstable airway in babies and infants. These cysts are rare, and early recognition may result in prompt cure. This condition is well described in the medical literature, although so far it has not been correlated with ciliopathies. Congenital saccular cysts are mucus filled and usually extend posterosuperiorly into the false vocal fold and aryepiglottic fold (the lateral saccular cyst). During anesthesia induction, low muscle tone may predispose to loss of airway due to obstruction. Cyst rupture during laryngoscopy is a potential risk, with subsequent loss of airway due to spillage of secretions and aspiration. Large bore suction should be readily available when securing the airway, as cyst content may be thick and difficult to suction.
Footnotes
Authors' Note
Jo Hegarty is now affiliated with Neonatal Intensive Care Unit, Auckland Hospital, New Zealand. Affiliated to the University of Auckland, New Zealand.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.