
Abstract
Intracranial complications secondary to chronic otitis media (COM) include otogenic brain abscess and sinus thrombosis. Intravenous antibiotics and imaging have significantly reduced the incidence of intracranial complications secondary to COM. However, the same does not apply to a developing country like Malaysia, which still experiences persisting otogenic complications. This case series describes 3 patients with COM and intracranial complications. All 3 patients had COM with mastoiditis, with 1 of the 3 having a cholesteatoma. Postulated reasons for the continued occurrence include poor access to health care, poor compliance with medication, and the lack of pneumococcal vaccination during childhood. In conclusion, public awareness and a timely specialty referral can reduce the incidence of intracranial complications of COM.
Keywords
Introduction
Intracranial complications secondary to chronic otitis media (COM) include extradural abscess, subdural abscess, meningitis (with or without encephalitis), otogenic brain abscess, and lateral or sigmoid sinus thrombosis. Age (first decade or elderly), immunosuppression, and presence of cholesteatoma are among the common influencing factors for the development of intracranial complications. 1
The availability of intravenous antibiotics and imaging methods has significantly reduced the incidence of intracranial complications secondary to COM. Moreover, mortality secondary to intracranial complications, especially otogenic brain abscess, has seen a steady decline over the years.
However, its severity and incidence remains high, more so in developing countries. 2,3 The World Health Organization in 2004 classified Malaysia and its neighbors in Thailand, Philippines, and Vietnam as nations with high prevalence of otitis media (<4%), Indonesia being on top at 5.4%. 2,4 A 3-year review at our tertiary referral center in Malaysia from 1998 to 2001 showed 9 (56%) of 16 patients had intracranial complications due to otogenic brain abscess, with lateral sinus thrombosis being the predominant complication. 5
A previous study done in the authors’ institution showed 13 patients underwent a mastoidectomy for a mastoid abscess secondary to acute or COM over a 6-year period from January 2002 to December 2007 . Mastoid abscess is a well-known extracranial complication of COM. 6
Objectives of this series are to review 3 cases with intracranial complications of COM presenting at the Ear, Nose and Throat (ENT) Department at University Kebangsaan Malaysia Medical Centre with the patient consent over the period of 12 months from July 2016 to June 2017. Discussion will include the pathophysiology and management of intracranial complications secondary to COM.
Clinical notes of the 3 cases were reviewed retrospectively and followed up over a course of 12 months post discharge. Only cases of intracranial complication of otitis media requiring admission, long-term antibiotics, and surgical intervention were selected. Chronic otitis media without intracranial complications were excluded from the study, for they are often treated as an outpatient.
Case 1
A 20-year old Malay male with right microtia and canal atresia (grade I) presented with a history of right otalgia. He was previously implanted with a bone-anchored hearing aid. He had purulent and foul-smelling ear discharge for 1 month. He was seen at the outpatients’ clinic but refused admission for intravenous antibiotics. This was succeeded by 1-week history of right temporal headaches, recurrent vomiting, expressive dysphasia, and low-grade pyrexia.
Examination revealed right external canal stenosis with keratin discharge. Neurological examination was unremarkable with intact cranial nerves. Pure tone audiogram recorded a moderate to severe conductive hearing loss at all frequencies on the affected ear.
A high-resolution computed tomography (HRCT) of the brain and temporal bone showed a soft tissue density originating from the right mastoid air cells with extension into the right middle ear and external auditory canal (EAC) representing a cholesteatoma (Figure 1). There was a concurrent right cerebellar abscess and epidural collection at the sigmoid fossa compressing on the fourth ventricle resulting in obstructive hydrocephalus.
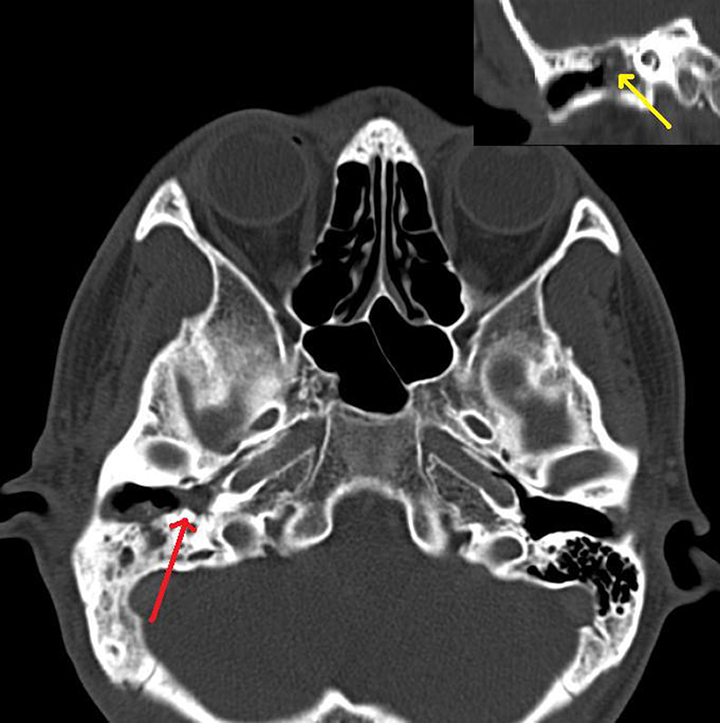
High-resolution computed tomography (HRCT) temporal with soft tissue density (cholesteatoma) originating from the right mastoid air cells with extension into the right middle ear. Coronal section (above right) showing disruption of ossicles (arrow) secondary to cholesteatoma.
He received a 2-week course of intravenous ceftriaxone and metronidazole and underwent a right modified radical mastoidectomy 24 hours post admission. Intraoperatively, there was cholesteatoma in the mastoid air cells, antrum, and EAC, partially eroding the promentary and lying over the oval window with destruction of the ossicles.
Microbial cultures were void of any growth. The brain abscess was treated conservatively due to it being <2.5 cm in the largest dimension with absence of midline shift. A postoperative magnetic resonance imaging (MRI) confirmed a right cerebellar abscess with perilesional edema (Figure 2), which resolved within 6 weeks of intravenous antibiotic administration.
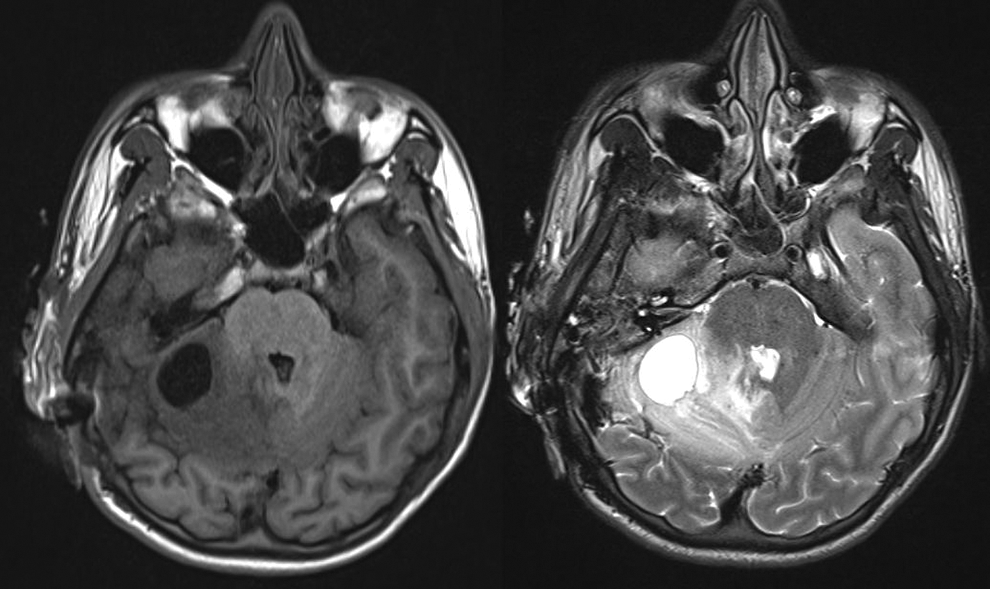
Magnetic resonance imaging (MRI): T1- (left) and T2- weighted (right) image of the brain indicating right cerebellar abscess with perilesional edema.
Case 2
A 23-year-old Malay gentleman with type 2 diabetes and poor glycemic control presented with progressively worsening right otalgia and neck swelling. He was initially treated for otitis externa with topical antimicrobial ear drops by his primary care physician. However, he was not compliant with follow-ups, and symptoms progressively worsened. Subsequently, he developed a foul-smelling purulent otorrhea 2 months later.
The ENT examination revealed a sagging posterior EAC with an aural polyp. There was also a 5 × 5 cm spherical, firm, and tender right level II neck swelling.
High-resolution computed tomography temporal bone revealed right mastoiditis with a right sternocleidomastoid (SCM) and superficial temporalis multiloculated abscess (Bezold abscess; Figure 3). Right sigmoid sinus thrombosis was present with evidence of filling defect with erosions of adjacent mastoid process. Pure tone audiogram revealed a right moderate conductive hearing loss. He was treated for a right acute supportive otitis media with mastoid, subperiosteal, and Bezold abscess.
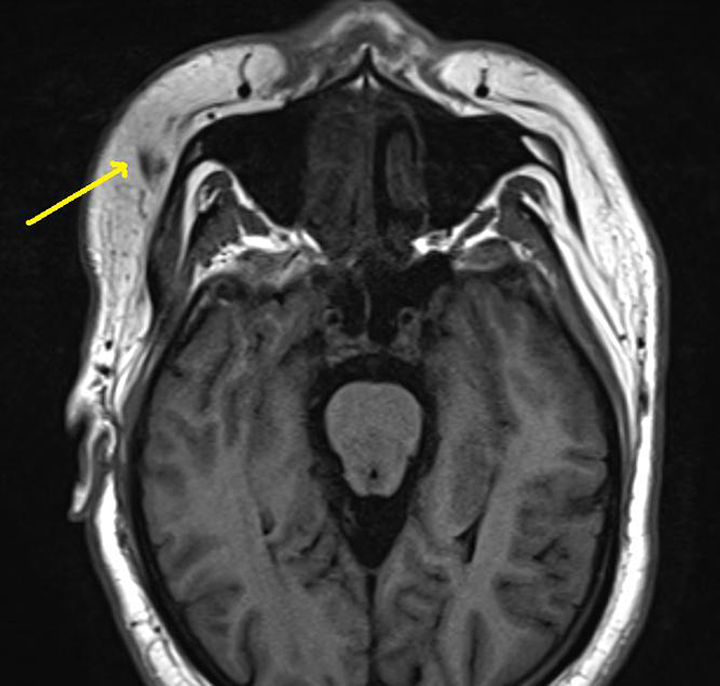
Computed tomography (CT) of the head showing right superficial temporalis multiloculated abscess (Bezold abscess).
A cortical mastoidectomy performed 24 hours later revealed a sagging fistulous posterior EAC wall with communication to the mastoid cavity and granulation tissue within the mastoid cavity, antrum, and middle ear. Concurrent incision and drainage of the Bezold abscess revealed an SCM abscess in communication with the mastoid tip. Tissue cultures grew Klebsiella sp. He was discharged well after receiving 2 weeks of intravenous ceftriaxone, vigorous wound toileting, and topical ear drops (framycetin sulfate 0.5%, dexamethasone 0.05%, and gramicidin 0.005%). He received a further 4 weeks of oral cefuroxime at home. Subsequent MRI of the brain showed resolution of sigmoid sinus thrombosis post antimicrobial treatment.
Case 3
A 30-year-old Malay female presented 2 years prior with right-sided headache, nausea, vomiting, generalized tonic–clonic seizures with no otalgia, otorrhea, or nasal symptoms. Otoscopic examination revealed a dull tympanic membrane. Both HRCT and MRI of the temporal bone showed right acute mastoiditis and temporal cerebritis with sigmoid sinus thrombosis. An emergency cortical mastoidectomy was performed and revealed granulation tissue at superior mastoid air cells, middle ear, and tympanic segment of the facial nerve as well as the tegmen and sinodural angle. She completed 2 weeks of intravenous ceftriaxone, followed by 4 weeks of oral cefuroxime on discharge. The seizures were controlled with phenytoin. She was not compliant with follow-ups and missed her post treatment imaging.
She presented a year later with fever, headache, and status epilepticus with no ear symptoms. Otoscopy was unremarkable with intact tympanic membrane. She underwent a right emergency cortical mastoidectomy and posterior tympanotomy. Granulation tissue was seen at the mastoid cavity, antrum, epitympanum, and tegmen mastoidea with erosion of the posterior cranial fossa but with an intact dura. Imaging revealed sigmoid sinus thrombosis with extension to the lateral sinus. She received another 2 weeks of intravenous ceftriaxone and a further 4 weeks of oral cefuroxime. On follow-up 12 months later, she was well with a dry ear.
Discussion
Sinus thrombophlebitis is caused by spread of infection to the inner wall of the venous sinus resulting in the formation of a thrombus via the action of fibrin and platelets, a process termed endophlebitis. Complete occlusion of the sinus may occur, and presence of organisms may promote the formation of an intrasinus abscess, whereby a septic emboli will have systemic manifestations in the form of septicemia. 1 Distal and proximal extensions may occur. Treatment is via eradicating the source of infection with little benefit from anticoagulants unless clots are extensive.
A poorly localized dull headache is a common sign among patients with intracranial abscess. 7 A triad of headaches, fever, and focal neurological symptoms were only present in 20% of patients. 8 A systematic review and meta-analysis done by Brouwer et al showed that the most common causative organism for brain abscess is Streptococcus sp followed by Staphylococcus sp, a trend observed to be similar across America, Europe, Africa, Asia, and Australia. 8 Fungi, parasites, and mycobacterium contributed to <2% of intracranial abscesses. Gram-negative organisms such as Klebsiella were relatively low at 4% in Asia, but certainly higher than that of America at 1.7%. Otogenic source was most common at 33% (otitis or mastoiditis) followed by sinusitis, meningitis, and odontogenic sources. 8
A study conducted by Tandon et al reported that the rates of otogenic brain abscess in the region of Liverpool, United Kingdom, had reduced significantly from 24.8% between 1950 and 1979 to 9.7% between 1980 and 2004 and believes that the increased use of antimicrobial therapy and prompt referral to ENT specialty in treating COM attributed to the decline in cases when compared to rhinogenic brain abscess. Mortality rates have significantly reduced from 47.2% in 1950 to 1979 to 5.8% in 1980 to 2004. Improved efficacy in antimicrobial therapy, better imaging, and improved intensive care therapy were contributing factors. 7
However, the same does not apply to Malaysia, a developing nation. There are still many otogenic brain abscesses seen in tertiary referral centers in Malaysia. To begin with, several of these cases were managed in the community or district. Not surprisingly, all 3 of our patients had COM with mastoiditis, with 1 of the 2 having a cholesteatoma.
Besides antimicrobial therapy, abscess drainage is still the mainstay of treatment and has not changed over decades. A transmastoid approach via a cortical mastoidectomy or modified radical mastoidectomy is carried out if there is imaging evidence of abscess communication to the mastoid or ear. Alternatively, a burr hole or craniotomy is performed if there is no evidence of communication. 9 Only large abscesses with local edema and hydrocephalus are drained, and smaller ones are often treated conservatively with antimicrobial therapy.
The authors postulate several reasons for the common presentation of intracranial complications secondary to COM in Malaysia compared to the reducing trend in several developed nations. First, many patients with COM do not seek medical treatment. Szyfter et al showed that chronic inflammation of the middle ear with cholesteatoma and/or granulation and not its acute stage contributed to 100 of 103 patients with otogenic brain abscess. 10 Patients in rural areas, many of whom are void of secondary and tertiary education, have poor insight into their condition and depend on traditional or herbal remedies for treatment. As a result, they may only consult a qualified medical practitioner as a last resort. A population-based survey in 2005 showed the prevalence of otitis media with effusion in Malaysia is prominent among rural areas, lower socioeconomic groups, and patients void of formal education. 3
This is the case of our first and third patient who sought medical attention for their discharging ear only after 1 month and a seizure, respectively. They often assume that an ear infection is always localized and were not aware that an ear infection may have a bacterial cause that if ignored may spread to the brain which is of close proximity.
Second, many patients in districts have poor access to health care, either clinics or hospitals. This is marked among patients from Borneo, East Malaysia, who depend on water transportation due to its hilly nature. Primary care case management programs have been suggested to increase the awareness of COM among primary care to reduce the rates of otitis media and its complications in developing countries. 11
Poor compliance with medication despite the availability of antimicrobial therapy makes the third factor. As evident in the third case, many patients do not understand the possible complications of COM and the close proximity of the ears to the brain. They often tend to stop antimicrobial therapy ahead of course completion when experiencing first signs of symptomatic improvement, thinking they are cured. Therefore, many will have untreated COM and harbor a cholesteatoma for a significant time. The assumption of a “safe COM” should be dismissed, and any COM should be treated with a possibility of intracranial extension in due time. 7 Antimicrobial resistance may not be a contributing factor, as most patients cultured aerobic and anaerobic organisms sensitive to readily available antibiotics such as cefuroxime and metronidazole.
Fourth, poor availability of imaging such as CT and MRI in districts has resulted in complications secondary to COM and mastoiditis being underdiagnosed despite a clinical suspicion, further delaying the referral to an ENT. 2,4 Contrasted CT is the modality of choice for assessing COM with intracranial complications. Magnetic resonance imaging was more superior to CT, especially in diagnosing smaller abscesses. 8 Imaging is essential in helping the surgeon to decide on which ear to operate on in bilateral ear disease; timing for surgical intervention based on edema, midline shift, and hydrocephalus; and best surgical approach based on size and position of abscess. Imaging modalities are also required for stereotactic aspiration off intracranial abscesses. 9
Fifth, Malaysia is lacking a prepaid national health-care plan or insurance. Patients not entitled to free public health care will have to pay for visits to primary care physicians, thus only seeing their clinician when their chronic condition is severe. Developed nations such as the United States with government-based health-care insurance have a better access to primary and preventative care, especially in the management of chronic diseases. 12 Having a regular primary care physician will allow other systemic illness such as diabetes to be monitored and controlled and reduce the rate of infections. A primary care physician is a first stop for many patients and will be able to educate and reinforce the importance of compliance to the patients. The financial burden will fall on patient and their families for treatment, and there needs to be earlier identification of COM, especially among children to void them from sequel of conductive and sensorineural hearing loss, which may lead to its own socioeconomic burden. 2
Sixth, pneumococcal vaccination is not mandatory in Malaysia. A randomized controlled trial involving 11 valent Streptococcus pneumoniae serotypes each conjugated to Hemophilus influenza-derived protein D vaccine or hepatitis A vaccine among 4968 infants showed a significant reduction of 33.6% in overall incidence of acute otitis media, with 57.6% due to pneumococcal serotypes and 35.6% for Hemophilus influenza serotypes. 13 Benefits of pneumococcal vaccination is not only limited to the ears but also to the lower respiratory tract; however, a mandatory inclusion of its vaccine will incur a large cost to the nation. There needs to be a population study into the disease and financial burden of pneumococcal infections in Malaysia. At present, the Malaysian goverment is mulling the need to have pnemococal vaccination as part of the national vaccine registry.
Conclusion
Although intracranial complications secondary to COM is declining in developed nations, developing nations such as Malaysia face a conundrum of its persistence due to patient factors such as poor compliance with treatment and insight into the complications of COM. Patient education, public awareness, and a timely specialty referral for COM may help in reducing the incidence of intracranial complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.