
Abstract
Objective:
To measure the current state of organizational and well-being factors in otolaryngology residency programs and associate these perceptions with demographics, pursuit of subspecialty fellowships, and performance on the Otolaryngology Training Examination (OTE).
Materials and Methods:
Anonymous mail and online survey study of otolaryngology residents from the Southern, Mid-Atlantic, and East South-Central Regions of the United States.
Summary of Results:
A total of 46 otolaryngology residents across 14 residency training programs (22% resident response rate) completed our survey. Residents who scored above the 80th percentile on the OTE perceived greater organizational support (median = 3.84) than residents who scored below the 40th percentile (median = 3.31), U = 48.00, P = .047, η2 = 0.14. Residents interested in fellowship reported less burnout (median = 2.44) compared to those who did not plan to pursue fellowship (median = 3.56), U = 105.00, P = .010, η2 = 0.05. Residents pursuing fellowship also reported less work–life strain (median = 2.56) than those forgoing fellowship (median = 2.89), U = 126.00, P = .044, η2 = 0.10. Residents with children reported greater work–life strain (median = 3.11) compared to those without (median = 2.56), U = 60.50, P = .008, η2 = 0.15.
Conclusion:
For otolaryngology residents in this survey sample, the perception of organizational support and well-being may influence resident performance (on OTE examinations) and ultimate career goals (fellowship applications). Program directors and coordinators can use this information to strengthen the perceptions of organizational support as well as improve the clinical learning environment to optimize training conditions for their residents. Residency program directors can also use the identified study measures to assess resident perceptions of the clinical learning environment and well-being for annual evaluation and improvement purposes.
Introduction
Surgical resident well-being has been increasingly recognized as a major focus in graduate medical education over the past decade. The recent emergence in 2015 of the Clinical Learning Environment Review from the Accreditation Council for Graduate Medical Education reminds medical educators that training occurs within an organizational context that has the power to either facilitate or hinder the professional development of physician trainees. As such, there is a need to understand and assess the current state of both resident well-being and perceptions of the clinical learning environment in graduate medical education. In an effort to fill this gap, our study identified several constructs that relate to the trainee and the environments in which they learn to better understand the current state of graduate medical education for otolaryngology residents.
While burnout, defined as “a syndrome of emotional exhaustion, feelings of depersonalization, and a lack of personal accomplishment, specifically in relation to one’s professional activity,” has dominated the conversation around resident well-being, other occupational health constructs such as resilience, work–life strain, and job satisfaction can also provide insight into the effects of work on an individual. 1 -3 Surgical specialties have long been recognized as stressful, with long work hours, extended residency training, mounting educational debt, and significant lifestyle repercussions. 4 -6 Among all medical education training programs, surgical residency is recognized as one of the most arduous. Increasing evidence suggests that burnout may impact the quality of patient care, including medical errors and patient satisfaction, yet surgical residency programs still struggle to improve resident well-being. 7 -10 Burnout, specifically emotional exhaustion, may contribute to the higher rates of surgical resident attrition at approximately 17% compared to other medical specialties. 6,11
Golub and colleagues 12 conducted a national study of otolaryngology–head and neck surgery (ENT) residents to understand factors associated with burnout during training. They found a prevalence of burnout among ENT residents, with 10% (n = 51) of residents reporting high burnout and 76% (n = 391) reporting a moderate level of burnout. Factors negatively associated with burnout included work–life balance, relationship stability, and career choice satisfaction. Furthermore, the desire for ENT residents to complete a fellowship has been found to be lower for senior residents, while the desire to not complete a fellowship is higher for senior residents compared to junior residents indicating the potential for fewer specialty trained ENTs in the workforce. 13 The difference in fellowship plans by training year suggests the clinical learning environment or experiences within graduate medical education are affecting residents’ intentions of pursuing fellowship training.
In a study of general surgery residents, a structured mentored program, allowing for either personal or professional support, was associated with significantly lower burnout. 14 Such findings, again, suggest that residents’ perceptions of organizational support and the clinical learning environment may influence well-being. In the current study, our objective was to measure the current state of organizational and well-being factors in surgical residency programs and detect any group differences based on demographics, career plans, and in-service examination performance. We predicted that greater well-being and better perceptions of the clinical learning environment would be associated with goals to apply for fellowship training and greater performance on the Otolaryngology Training Examination (OTE) or in-service examination for ENT residents.
Materials and Methods
Between March 2016 and June 2016, surgical trainees from general surgery, neurosurgery, otolaryngology, plastic and reconstructive surgery, orthopedic surgery, and urology were recruited to participate in a larger research agenda approved by our institutional review board. Respondents ranged across all training years and were from the South Atlantic (District of Columbia, Delaware, Florida, Georgia, Maryland, North Carolina, South Carolina, Virginia, and West Virginia), Mid-Atlantic (New Jersey, New York, and Pennsylvania), and East South-Central (Alaska, Kentucky, Mississippi, and Tennessee) regions. For the purpose of the current research question, we focused on the data related to ENT residents.
Resident well-being was measured through predominately validated scales, Maslach Burnout Inventory–shortened 9 items (Mind Garden, Inc, Menlo Park, California), 3,15 Brief Resilience Scale–6 items, 16 Work/Social Conflict Scale–9 items, 17 and Job Satisfaction Scale–5 items. 18 Clinical learning environment measures included the Abbreviated Workplace Climate Questionnaire–9 items 19 and the Short Survey of Perceived Organizational Support–16 items. 20 Burnout was measured using a 7-point Likert-type scale (1 = never, 7 = everyday). Resilience, job satisfaction, workplace climate, and perceived organizational support were measured on a 5-point scale (1 = strongly disagree, 5 = strongly agree). Work–life strain was measured using a 5-point frequency scale (1 = never, 5 = always). Across scales, some items were reverse-coded and were tailored slightly to fit our study context. While burnout is typically assessed through 3 domain areas (ie, emotional exhaustion, depersonalization, and personal accomplishment), our study created one composite score through a shortened survey (3 items for each of the 3 domains) based on the need to reduce survey length to avoid survey fatigue.
Respondents reported their approximate percentile score on the most recent in-service examination (OTE) through 5 range categories. As this survey was distributed to all surgical trainees in the region, percentiles were utilized instead of stanines. High and low in-service performance was categorized, with scores above 61st percentile as “high” and scores below the 40th percentile as “low.” Demographic items included gender, training year, parental status, and fellowship plans.
Residency program directors were directly e-mailed through Qualtrics (Qualtrics LLC, www.qualtrics.com) and asked to either (1) provide 15 minutes during a resident-specific meeting to distribute a paper version of our survey or (2) forward an electronic survey link to current residents in their training program. For paper survey data collections, residency program coordinators were mailed study materials including paper surveys, an instruction sheet, a data collection script, and a prepaid envelope to return the completed surveys within 3 weeks. Training programs at our home institution allowed a member of the research team to collect the data on behalf of the program coordinator. A data collection script outlining the study purpose was read aloud during distribution of paper surveys and provided in written form when the survey was taken online. Residents were able to turn in a blank survey or withdraw from the online survey, if they chose not to participate without negative consequences. All submitted paper surveys were sealed in a prepaid envelope and mailed back to the research team.
All analyses, including descriptive statistics and bivariate correlations, were conducted through IBM SPSS Statistics 24 (IBM, Armonk, New York). Group comparisons for fellowship plans (yes and no) and in-service performance (high and low) were analyzed through Mann-Whitney U tests with composite mean scores for each construct. Each significant comparison also had a η2 effect size calculated to better understand the size of the difference (small = 0.01, medium = 0.06, and large = 0.14).
Results
A total of 46 (22% response rate) ENT residents out of 209 across 14 training programs completed our survey (Table 1). Three program directors allowed paper survey data collection, while 11 additional program directors forwarded the electronic survey to their current residents.
Participant Demographics.
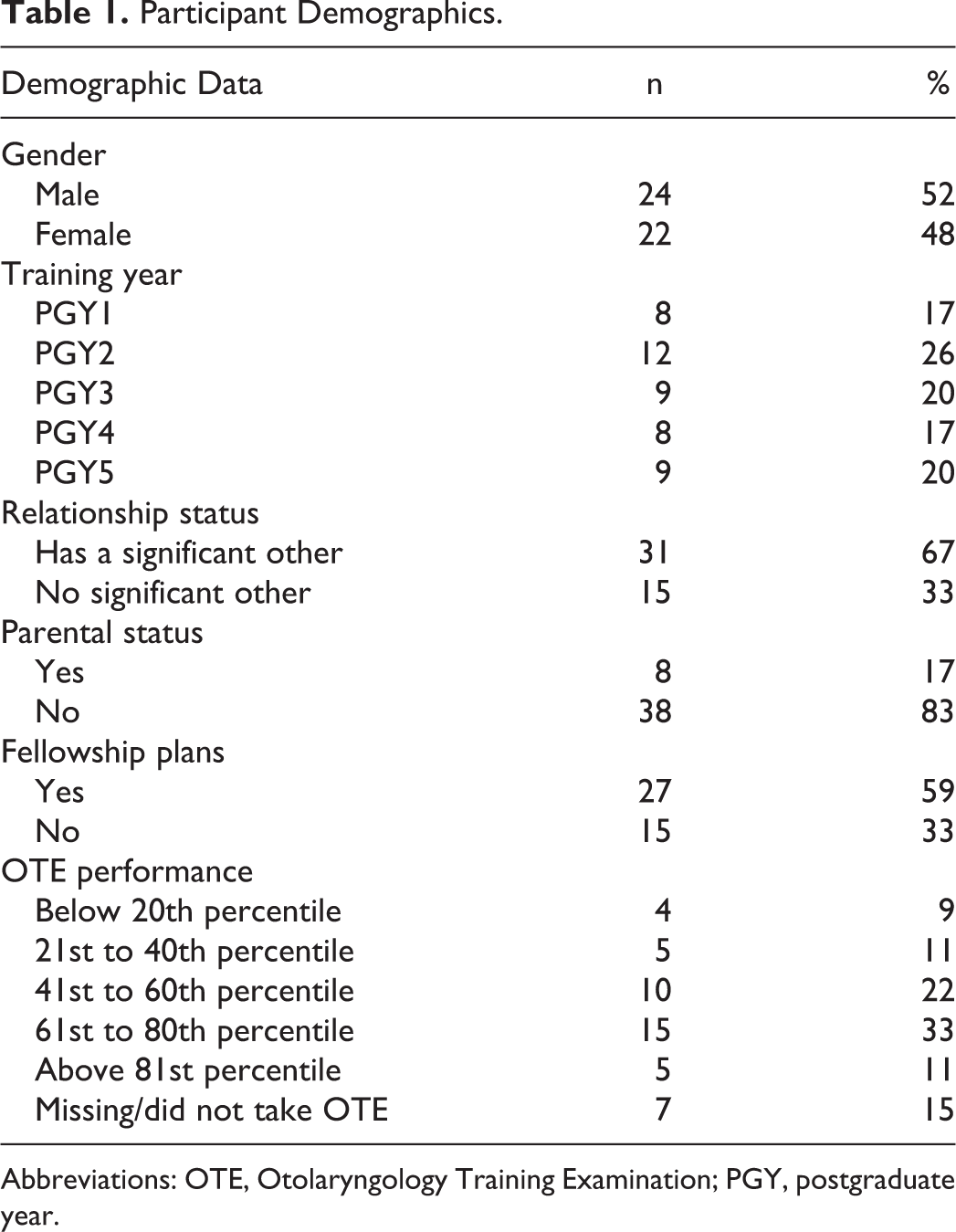
Abbreviations: OTE, Otolaryngology Training Examination; PGY, postgraduate year.
Scale reliabilities ranged from adequate to excellent internal consistencies (Table 2). One job satisfaction item was removed from composite score calculations based on item scale reliabilities, “I worry about making enough money as a surgeon.” Point-biserial correlations (Table 2) indicated a positive relationship between OTE performance and perceived organizational support, r pb = .43, P = .019, (0 = low, 1 = high). Fellowship plans had a negative relationship with burnout, r pb = −.39, P = .010, and work–life strain, r pb = −.34, P = .027, (0 = no, 1 = yes). Parental status had a positive relationship with work–life strain, r pb = .41, P = .005, (0 = no, 1 = yes). While there was a correlation between gender and resilience, the group comparison analysis did not reveal any significant relationship between the 2 variables.
Correlation Matrix, Means, Standard Deviations, and Scale Reliabilities.a
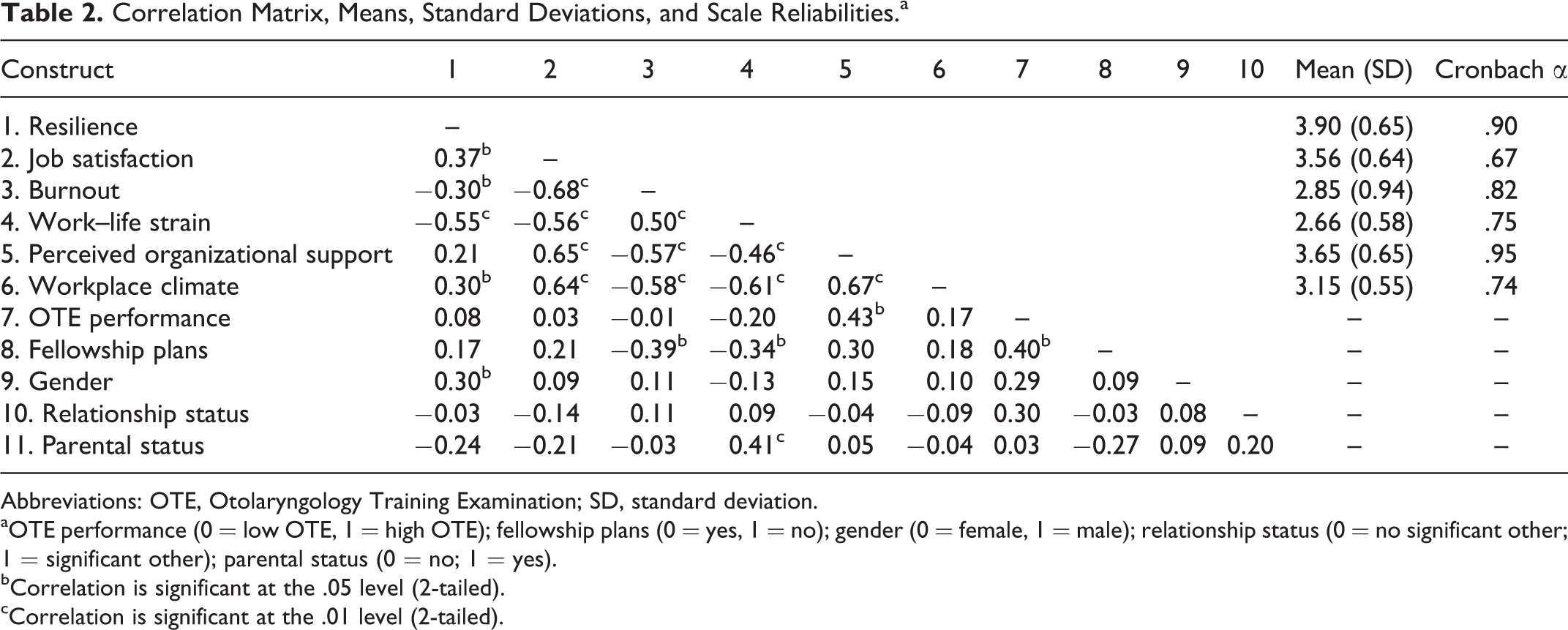
Abbreviations: OTE, Otolaryngology Training Examination; SD, standard deviation.
aOTE performance (0 = low OTE, 1 = high OTE); fellowship plans (0 = yes, 1 = no); gender (0 = female, 1 = male); relationship status (0 = no significant other; 1 = significant other); parental status (0 = no; 1 = yes).
bCorrelation is significant at the .05 level (2-tailed).
cCorrelation is significant at the .01 level (2-tailed).
There were no significant differences between ENT residents with and without significant others or by gender for the well-being and clinical learning environment constructs. The only construct that varied between high and low OTE performers was perceived organizational support. Those who scored above 60th percentile on the OTE perceived greater organizational support (median = 3.84) than ENT residents who scored below the 40th percentile (median = 3.31), U = 48.00, P = .047, η2 = 0.14. There were also differences in burnout and work–life strain between ENT residents interested in pursuing fellowship training compared to those who did not plan to pursue fellowship (Table 3). Specially, ENT residents interested in fellowship reported less burnout (median = 2.44) compared to those who did not plan to pursue fellowship (median = 3.56), U = 150.00, P = .010, η2 = 0.05. The ENT residents pursuing fellowship also reported less work–life strain (median = 2.56) than those forgoing fellowship (median = 2.89), U =126.00, P = .044, η 2 = 0.10. The ENT residents with children reported greater work–life strain (median = 3.11) compared to those without children (median = 2.56), U = 60.50, P = .008, η2 = 0.15.
Group Differences on Well-Being and Perceptions of Clinical Learning Environment Based on Fellowship Plans and OTE Performance.a
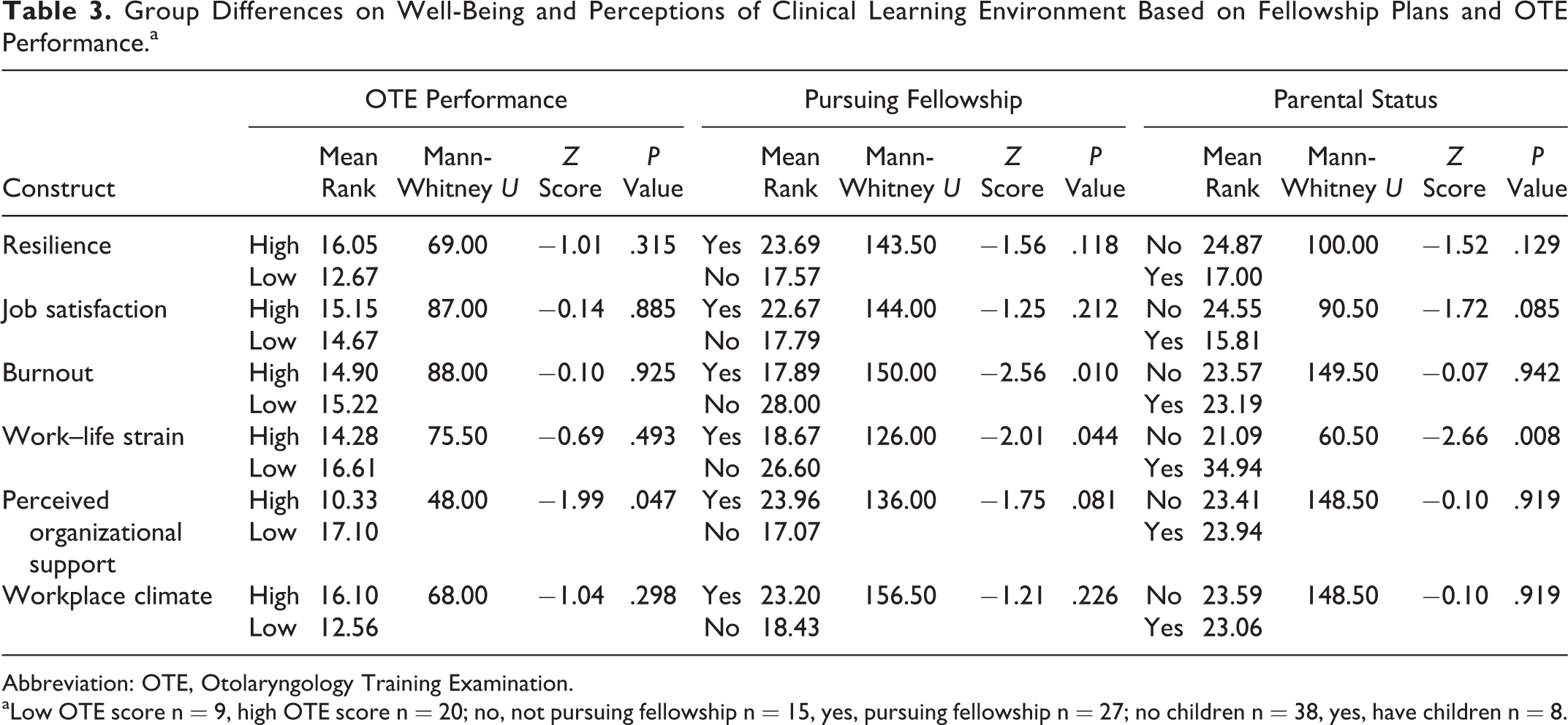
Abbreviation: OTE, Otolaryngology Training Examination.
aLow OTE score n = 9, high OTE score n = 20; no, not pursuing fellowship n = 15, yes, pursuing fellowship n = 27; no children n = 38, yes, have children n = 8.
Discussion
Our study is the first to utilize a wide array of measurement tools to gauge ENT resident well-being and perceptions of the clinical learning environment in otolaryngology. While personal factors can affect well-being, it is increasingly recognized that poor well-being is a systemic problem of the health care and medical education training environment. 21,22 Our findings suggest that otolaryngology residents with higher OTE scores perceive greater support from their programs and institutions, while those interested in fellowships perceive less work–life strain and less burnout, and residents with children experience greater work–life strain overall during residency than those without children.
Improving the perception of the clinical learning environment by enhancing perceived organizational support may help bolster resident performance on the in-service examination. Residents, and particularly otolaryngology residents, are high achievers with typically higher than average scores on USMLE and other standardized testing. Given the stressors of the clinical learning environment and the minutia that often appears on this examination, there can be significant variation in performance between residents and between postgraduate years. Residents who perform in the bottom quartile on the OTE are at significantly higher risk of failing the ABO Written Qualifying Board examination. 23 Perceived organizational support is an established construct in organizational psychology that is broadly described as an institutional factor that affects many individual psychosocial factors including job satisfaction and burnout. 24 -27 On an individual level, perceived organizational support is your perception that the organization values your contributions, well-being, and will provide resources to allow you to function in your role and overcome any crises that may occur. 24,26 This differs from workplace climate that explores the perception of personal autonomy, workload, and support of your coworkers in your organization. 24 Unlike perceived organizational support, measures of workplace climate, job satisfaction, work–life strain, burnout, and resilience did not differ between those who reported excelling on the OTE and those with below-average scores.
Perceived organizational support at the departmental level can be influenced by the program director and chair, while at the institutional level the GME community can play a vital role. At the departmental level, enhancing the perception of organizational support can occur by establishing an educational subcommittee that includes resident representation, increasing positive feedback and/or recognition for personal accomplishments, educational resources (eg, resident textbook stipends or a resident library), increasing electronic resources (provision of tablets, e-books, access to review question banks), formal or informal OTE review preparation, or establishing formal or informal mentorship programs. Implementation of a learner-centered educational curriculum has been shown to improve OTE performance, 28 and preliminary data suggest that incorporating app-based learning into otolaryngology training programs may lead to improved performance on knowledge-based assessments. 29 At the institutional level, perceived organizational support may be enhanced by increased resident participation on institutional committees within the hospital (eg, Resident Work/Life committees), developing institutional educational resources that benefit all house staff, providing well-being activities at the GME level (gym memberships, child care resources, social events), providing a common space for educational pursuits, and promoting “back to bedside” activities with incentivized participation, 30 among others. The provision of academic resources may relate to better resident wellness and improved perceptions of the clinical learning environment in surgical residency programs. 24 Specifically, educational stipends, review question access, in-service board preparation, and additional support for those with poor performance correlated with positive perceptions of the clinical learning environment and resident well-being. 24
While pursuit of advanced subspecialty fellowship training is not the goal for all residents, it is the responsibility of both the program director and the Institutional Graduate Medical Education office to ensure the clinical learning environment is optimized to support fellowship training if that career path is chosen by the individual. Our survey study suggests that for fellowship pursuit, work–life strain and burnout are 2 areas that can be targeted in the clinical learning environment. Work–life strain was also significantly greater for residents with children overall than for those residents without children. Considering the additional burden, socially, financially, and educationally extending additional postgraduate years as a trainee, those experiencing less burnout and a currently favorable state of work–life balance are more apt to continue their training to subspecialty fellowship.
Work–life strain occurs when the often competing interests and time requirements of work life and personal life conflict and place strain on the physician. 31 While much of the research aimed at reducing this work–life strain has focused on taking time off from work or maximizing lifestyle outside of work (eg, duty hour regulations, social events outside of work, child care access), the missing link may be finding connection and belonging at work as a way to mitigate strain. 32,33 These authors argue that addressing burnout and work–life strain can only occur when one finds fulfillment from work and not only when escaping from it. 33 Relationships between fellow residents, patients, and family members may suffer when learners are urged to disconnect from the core tenets of professionalism, compassion, and humanism in order to achieve work–life “balance.” 33,34 In the spirit of promotion of well-being, many times residents are now encouraged to leave work so that they can enjoy life, rather than finding pleasure and meaning in the patient care and scholarship that exists in the graduate medical education environment. To be effective, work–life strain initiatives must highlight the connection between the medical profession and personal growth, as well as promoting wellness outside of the hospital. 33 Specific suggestions that may help residents, especially residents with children, include access to child care, stress management both inside and outside of the hospital, encouraging exercise, offering gym membership and access at off-peak hours, and a variety of social and bonding experiences with house staff and faculty. In addition, program allocation of protected time and space for resident-only meetings to share experiences and discuss themes of resilience, rather than a formal resilience curriculum, can be highly effective. 33 Effective mentoring programs that support both the professional and the psychological and social aspects of residency, taking into consideration mentee priorities, are the most successful. 33,35 Peer mentoring programs have also been shown to be very effective to connect residents to their work and enhance the feeling of belonging in the community of learners, thereby potentially alleviating some degree of work–life strain. 33,35
Otolaryngology residents who were not interested in pursuing advanced fellowship training also perceived higher levels of burnout. Confronting and targeting burnout is a high priority not only for program directors and institutions but for the medical community at large. In a study of otolaryngology residents in 2007, Golub et al found that burnout was extremely common, with high or moderate levels at 86%. 12 The strongest factor in this study was hours worked, being predictive of emotional exhaustion; burnout was higher in otolaryngology residents than otolaryngology chairs or faculty. 12 Recent research in this field suggest that the origins of burnout in resident trainees in general are rooted in the clinical learning environment. 36 The aspects of the learning environment implicated are long working hours, lack of autonomy, lack of reciprocity, supervisory support, teamwork, and relationships between supervisors and other allied health professionals. 12,36 -38
To curb and address burnout in our otolaryngology residency programs, we need to introduce more flexibility into our training paradigms. Residents enter our training programs from diverse backgrounds, with a wide range of lifestyles and priorities both inside and outside of our programs. If we are able to reduce the systemic inefficiencies (eg, reducing clicks in the electronic medical record) and burdens of tasks that are better assigned to nonphysicians (eg, the increased use of advanced practice professionals who can shoulder some of the inpatient floor busy work burden, improving administrative support for scheduling and other administrative tasks), then residents can engage in more bedside patient care and technical skill acquisition that provide enhanced individualized professional identity and meaning to being a physician. As less physical activity has been correlated in otolaryngology residents with decreased quality of life and increased burnout, 39 efforts to combat burnout should include a focus on personal wellness in both the physical (diet and exercise) and the mental (relaxation, stress reduction, coping strategies). A recent systematic review and meta-analysis of controlled interventions to reduce burnout in physicians found that organization-directed interventions were more effective than physician-directed interventions at improving burnout scores. 40 Organizational interventions that were most effective combined multiple strategies, such as structural changes, fostering communication between team members and fostering a culture of teamwork and autonomy. 40 All physician-directed interventions led to small yet significant improvement in burnout with no differences between the type of intervention (mindfulness, improving communication or coping skills, and so on). 40 Overall, it would seem prudent to incorporate both interventions—the organizational intervention from the institutional perspective and the physician directed from the program perspective to make the most impact on reducing burnout and improving well-being.
The strengths of our study include the use of validated measures to assess well-being and the perceptions of the clinical learning environment to start a discussion around how these factors relate to medical knowledge metrics during residency and the pursuit of additional training in the form of subspecialty fellowship after residency. Limitations of the study include the survey-based methodology, which is hindered by response rate, potential of social desirability, recall bias, and selection bias. The nature of the cross-sectional survey methodology can only infer correlations but do not allow us to infer causation. Further studies of surgical resident well-being and how the clinical learning environment can evolve to better promote outcomes for both the patient and the surgeon will be essential for our future generations.
Conclusion
Resident well-being is the most important topic in graduate medical education today. The influence of the clinical learning environment on well-being is now being increasingly recognized. Our study is an important first step to further elucidate the relationship of resident well-being and organizational factors in the clinical learning environment. Physician well-being, and specifically surgeon well-being, is a high priority to nurture future generations of our profession that places caring for others as the highest priority.
Footnotes
Authors’ Note
Presented as oral presentation at Triological Society Annual Meeting at COSM, National Harbor, MD, USA, on April 21, 2018.
Acknowledgments
The authors wish to thank all of the otolaryngology program directors, program coordinators, and residents who participated in our study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.