
Abstract
Background:
Foreign body aspiration (FBA) is a major cause of morbidity and mortality in children. It is a preventable event that predominates in preschool age. The signs and symptoms mimic respiratory diseases common in the same age-group. We compared FBA in infants to FBA in older children.
Methods:
Retrospective analysis of all the cases of suspected FBA of children under the age of 18 years hospitalized at one medical center during 2002 to 2016. We analyzed the data according to age: up to 1 year (infants) and 1 to 18 years.
Results:
One hundred seventy-five children with suspected FBA were admitted; of whom, 27 (15%) were infants and 148 (85%) were older children (age 1-18 years). For the 2 age groups, adults witnessed 85% and 73%, respectively, of the incidents (P = .4). In the neonate group, 48% presented with normal X-ray findings compared to only 20% in the older group; 15% of the older group had a positive chest X-ray for a foreign body, while none had such in the infants’ group (P = .01). For the 2 age groups, the majority of the FBs found were from organic origin. About half of the patients were diagnosed and managed within 24 hours of the aspiration event. In 10%, repeated bronchoscopy was performed due to a retained FB remnant. In a multivariate analysis, signs and symptoms (P < .05), location of the FB (P < .001), and witnessed aspiration (P < .001) were independent prognostic factors for the length of hospitalization.
Conclusion:
Foreign body aspiration is not uncommon in young infants; the management is challenging due to small airways, the need to use smaller bronchoscopes, and the lack of working channel forces in pediatric bronchoscopes.
Introduction
Foreign body aspiration (FBA) is a major preventable cause of morbidity and mortality in children, being the fourth leading cause of accidental death in children younger than 3 years and the third in infants under 1 year. 1 Sources of foreign bodies (FBs) vary among populations, 2 although the majority of FBs aspirated in children are of organic type. 3 -7
Foreign body aspiration predominates in preschool age, 2 especially in children under the age of 3 years. 1,3,5,8,9 Inadequate observation by adults, together with the tendency of children to explore the environment through their mouths, allows access to small objects, which sometimes results in aspiration. 3 Other contributing factors include the inability to chew food, inadequately developed posterior dentition, and immature neuromuscular mechanisms of airway protection. 4,8,10
The signs and symptoms of FBA are mainly respiratory and can simulate diseases such as asthma or croup, delaying correct diagnosis and contributing to morbidity and mortality. 8 The majority of studies of FBA evaluated children under age 3 years and did not focus on infants (under the age of 1 year). In this study, we analyzed the cases of FBA in infants, to investigate particular characteristics, compared to children aged 1 to 18 years.
Methods
Data Collection and Selection Criteria
This is a retrospective analysis of all the cases of suspected FBA of children below the age of 18 years who were admitted to Rambam Medical Center (RMC) between January 2002 and December 2016 and who underwent rigid bronchoscopy. As the largest tertiary referral center in northern Israel, RMC offers the full range of pediatric subspecialties, including pediatric intensive care and pediatric pulmonology. Rambam Medical Center serves a heterogenous population that includes Jews, Arabs, and Druze.
From the medical records, we collected data regarding demographics (age and gender), symptoms, duration of symptoms prior to diagnosis, physical examination, radiographic findings, findings on bronchoscopy, the need for a second intervention, and complications. We analyzed the data according to 2 age groups: up to age 1 year (to which we referred as the infants’ group) and 1 to 18 years (to which we referred as the children’s group). Indications for bronchoscopy were a suggestive history of FBA and suspicious findings in physical examinations or from chest X-rays.
Patients underwent bronchoscopy under general anesthesia. Induction was performed using propofol (3 mg/kg) and/or sevoflurane inhalation using a mask. The vocal cords and trachea were sprayed with lidocaine 2% under direct laryngoscopy. During endoscopy, all children were in spontaneous respiration and breathed with high rates of oxygen (>50%) through a Waters circuit connected to the side arm of the rigid bronchoscope. Anesthesia was maintained with propofol (from 6 to 10 mg/[kg·h]) associated with remifentanil (0.02-0.2 µg/[kg·min]).
The FBs were removed using age-appropriate rigid ventilating bronchoscopes (Karl Storz, Tuttlingen, Germany) equipped with optic telescopes (Hopkins, Tuttlingen, Germany). Alligator or peanut-type forceps were used as needed for grasping. We were able to use the optic telescope forceps only at bronchoscope size 3.5 (Karl Storz) and above. When remnant FBs were suspected clinically, a flexible bronchoscopy was performed, and when the result was positive, the patients underwent another rigid bronchoscopic procedure.
Statistical Analysis
We examined a number of variables for their association with duration of hospitalization. Variables that had prognostic potential on univariate analysis were subjected to multivariate analyses with the Cox proportional hazards regression model. The analyses were performed on JMP 10 software (SAS Institute Inc, Cary, North Carolina) and confirmed by an independent statistician on an IBM SPSS Statistics package (IBM Corporation, Armonk, New York). All P values were 2 sided, and a P value of less than .05 was adopted as the threshold for statistical significance.
Results
During the study period, 175 children with suspected FBA were admitted to our institution; of whom 27 (15%) were infants (below 1 year) and 148 (85%) were older (aged 1-18 years). The proportion of males was similar in the 2 groups: 59% (16) and 64% (95), respectively, P = .68. Respective mean ages were 10.8 months, with a range of 6 to 12 months, and 4.2 years, with a range of 1.1 to 18 years. The majority of the aspiration events were witnessed by adults in both age groups—85% and 73%, respectively (P = .4). Patients’ demographics are presented in Table 1.
Patient Demographic Characteristics and Features of the Events.
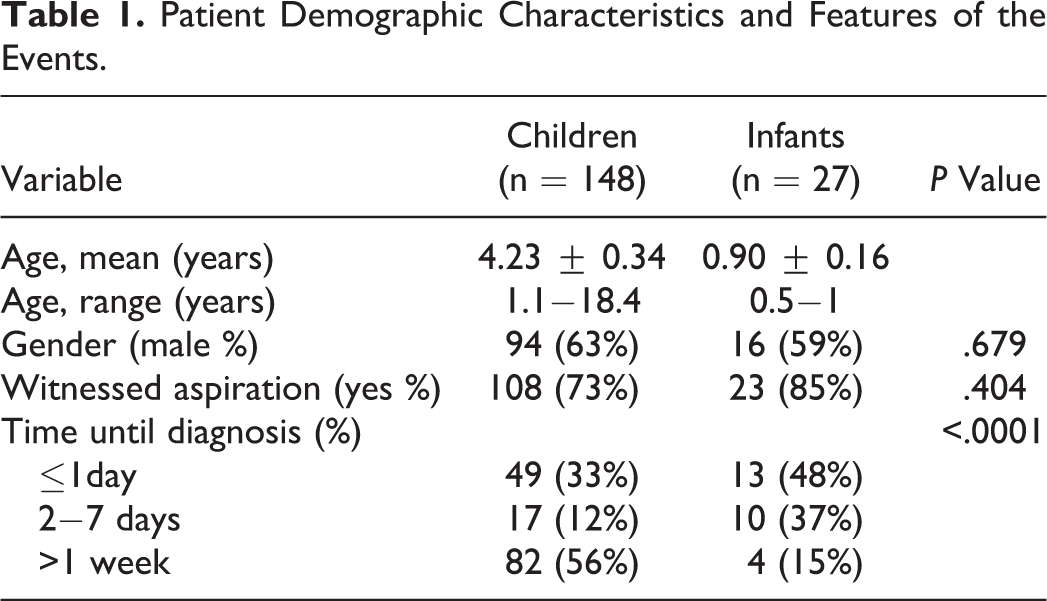
Table 2 summarizes the signs and symptoms for both groups at presentation. In the infants’ group, the most prevalent symptoms were cough (48%) and dyspnea (22%). Rales on auscultation were the most common physical signs, followed by decreased breath sounds. In contrast, in the older group, decreased breath sounds were the most prevalent sign, followed by wheezing.
Clinical Presentation and Radiographic Findings on X-ray.
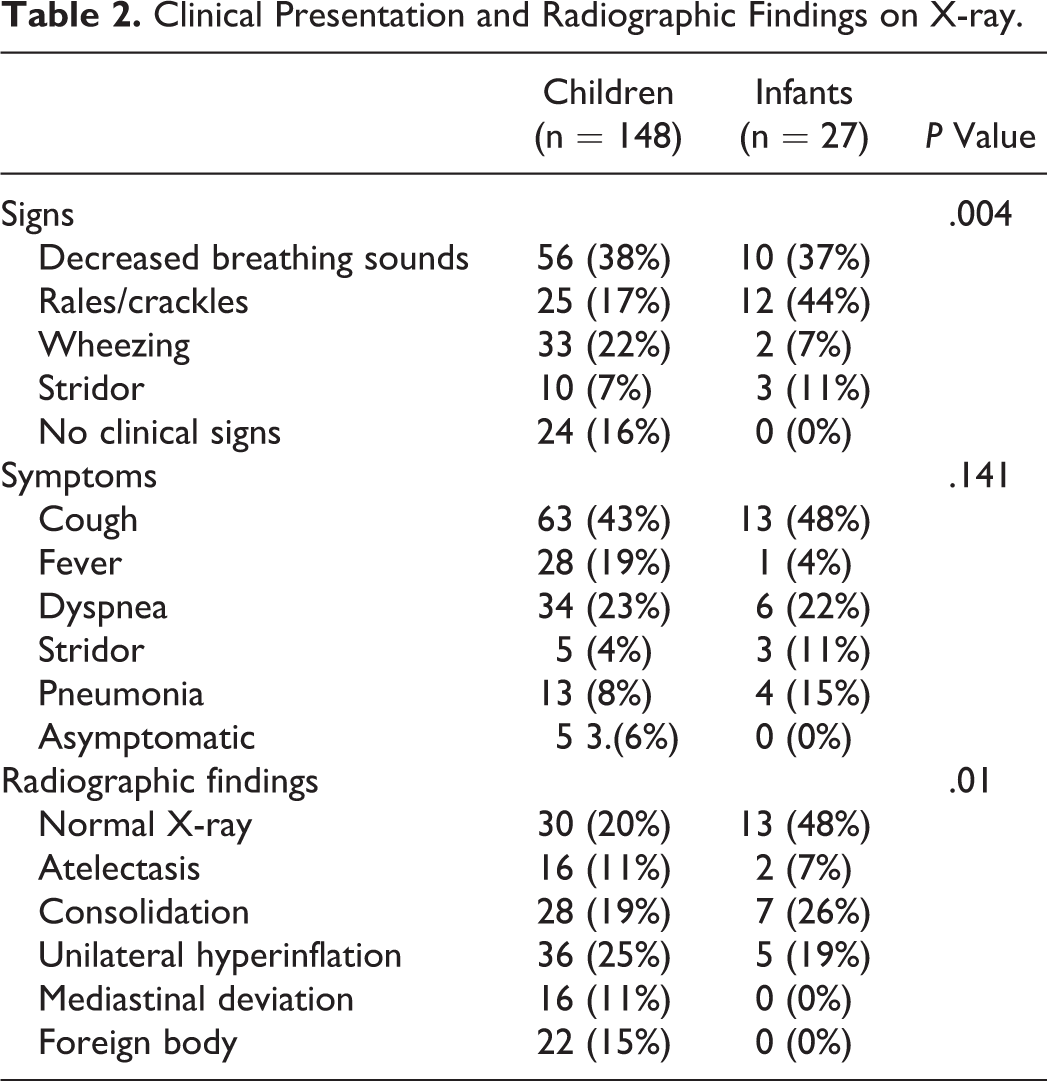
Chest X-rays were performed for all patients included in the study. For some, this was done to exclude other possible differential diagnoses that could explain the symptoms, and for the remaining, the aim was to identify specific findings that could elucidate the nature or the site of the FB. In the infants’ group, 48% presented with normal X-ray findings compared to only 20% in the older group; 15% of the latter had a positive chest X-ray for a FB, while none had such in the neonatal group (P = .01). One-sided consolidation was seen in 26% and 19% of the examinations for the younger and older groups, respectively, and unilateral hyperinflation in 19% and 25%, respectively (Table 2).
For the 2 age groups, the majority of the FBs found were from organic origin. Nuts and seeds were found in 26% and 22% of neonatal cases, respectively, compared to 43% and 13% in the older group. In 15% of infants, no FB was retrieved during the bronchoscopy compared to only 8% in the older group (Table 3). None of these patients had to undergo another bronchoscopy since they were asymptomatic during their hospitalization and none had postoperative complications. Table 3 presents the locations of the FBs, the majority were found in the right main bronchus in the infants (30%) and in the left main bronchus in the older group (42%).
Types and Locations of the Foreign Bodies.
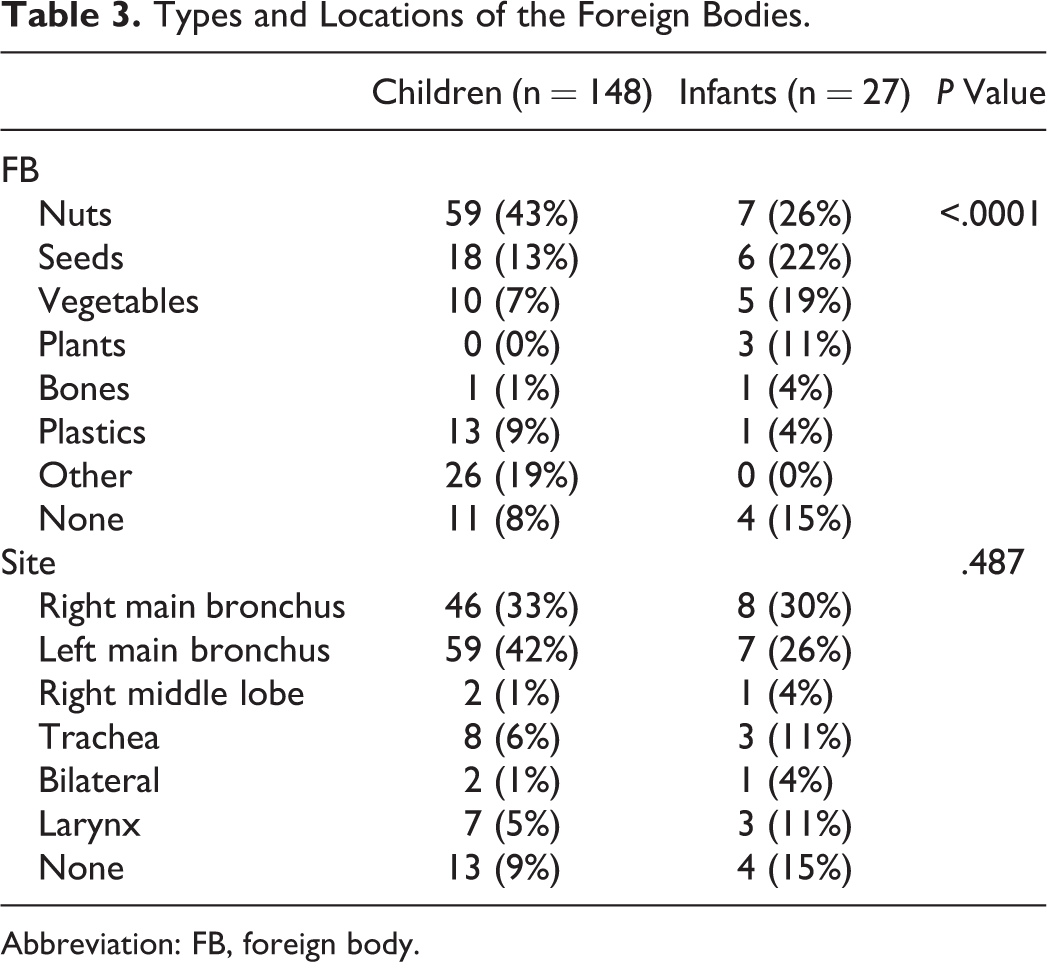
Abbreviation: FB, foreign body.
In 3 infants, a second bronchoscopy was performed due to unrelieved symptoms. In a 9-month-old infant, remnants of the FB (seeds) were retrieved from the left lower lobe 5 days after the initial procedure. The second infant was a 6-month-old who aspirated nuts. He underwent a second bronchoscopy that showed significant edema and remnants of the FB in the right lower lobe, which were removed. The third was an 11-month-old who aspirated nuts and presented to the emergency department 14 days after the event. The FB body was removed by rigid bronchoscopy, but a repeated bronchoscopy 1 week later showed granulation tissue and remnants of FB in the left lower lobe. The 3 failures described were initially performed by size 3 bronchoscope without using optical forceps.
Three infants had complications after the procedure, all were managed successfully. One patient required mechanical ventilation after the bronchoscopy due to severe subglottic edema, one had pneumothorax, and in one, desaturation occurred after the procedure and the patient was admitted to the pediatric intensive care unit for observation.
Five patients in the older group had to undergo a second bronchoscopy due to failure of the first procedure. In 2 of those cases, the FB was covered by granulation tissue and secretions and was retrieved later during the hospitalization. One child had to be admitted to a pediatric intensive care unit following a laryngeal edema that was observed during the procedure and desaturation.
No deaths were identified in either group. The mean hospital stay was 3.2 days (range: 1-14 days) with 10 (37%) of 27 discharged within 1 day of admission in the neonatal group. In the older group, 49 (33%) were discharged 1 day following hospitalization, and the mean hospital stay was 2.9 days (range: 1-27 days), with no statistically significant difference between the groups (P = .67).
In a multivariate analysis of the entire cohort (Table 4), signs and symptoms (P < .05), location of the FB (P < .001), and witnessed aspiration (P < .001) were independent prognostic factors for the length of hospitalization. The type of the FB was not associated with the duration of the hospitalization (P = .6).
Multivariate Analysis of Factors That May Be Associated With Longer Hospitalization.
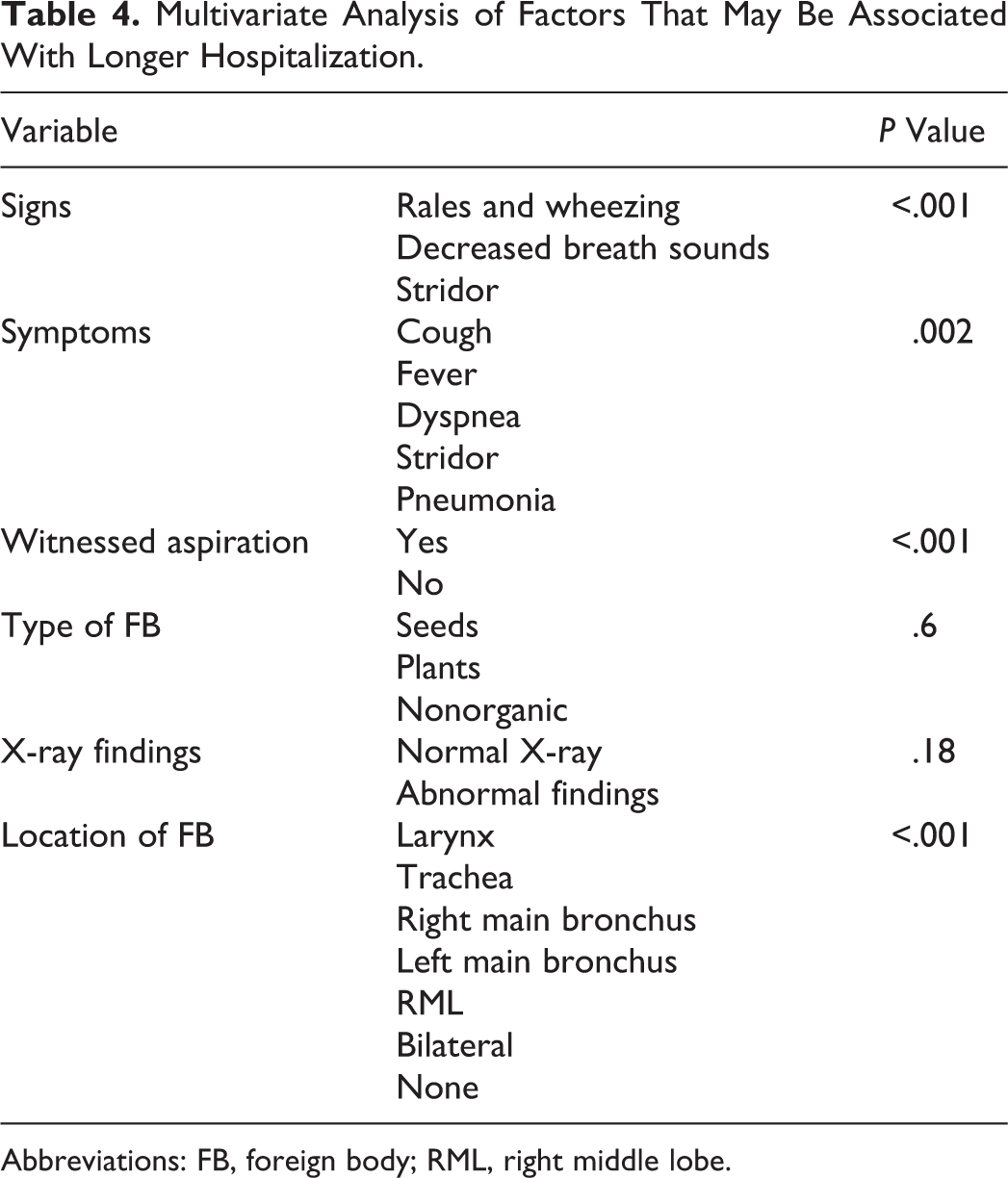
Abbreviations: FB, foreign body; RML, right middle lobe.
Discussion
Foreign body aspiration in children is an accidental event and if misdiagnosed can result in serious morbidity and mortality. It is most prevalent in the preschool age. 1,3,5,8,9
Of the children who were admitted to our institution with FBA during the study period, 16% were under the age of 1 year. Infants under age 1 year constituted 24% of children under the age of 3 years, which is higher than the proportion described in another cohort (14%). 3 The relatively high incidence of FBA in infants at our medical center, compared to other studies, may be due to cultural characteristics of our population. For example, the large proportion (44%) of infants who aspirated peanuts and seeds indicates a lack of awareness among many adults in our population to keep seeds away from infants and also reflects the Middle Eastern custom of eating seeds and nuts at social events. In an effort to encourage infants to taste new types of food, parents may give them foods that they are not yet able to chew and swallow appropriately, and this may cause them to aspirate. In our series, feeding an inappropriate food was a more common reason for aspiration than was lack of supervision and infants’ unintentional swallowing. On the other hand, adults may not pay enough attention to babies’ grabbing from tables, seeds and nuts served to adults. Considered together, these data demonstrate a need to educate caregivers of young children, with the aim of reducing events of FBA. Such education can be given by pediatricians or nurses at maternal and child health centers and should emphasize the importance of giving infants the appropriate type of food according to their age and should guide them how to act in case of aspiration. Training and educating parents have been shown to result in a decrease in cases of FBA in infants. 11,12
In the current study, the ratio of males to females was 3:2, which is consistent with other studies that reported male predominance. 3,4,7 One possible explanation is the more adventurous nature of boys, though this may be less obvious at the age of infancy.
Among our infant patients, 85% of the events were witnessed by adults. Adult witness facilitates clinical workup and prevents delayed diagnosis, which is of high importance since the signs and symptoms of FBA simulate a number of pediatric diseases such as bronchiolitis, pneumonia, and asthma. Despite the high rate of adult witness, only 48% were diagnosed within 24 hours. This can be explained by the lack of awareness by the caregivers and primary care physicians of the possibility of aspiration in this age-group. Among our patients aged 1 to 18 years, 73% of the events were witnessed by an adult. Children above the age of 1 year are sometimes left without tight observation, while infants under the age of 1 year are kept under constant adult supervision and rarely left alone. Taken together, the high proportion of witnessed aspirations in both age groups apparently contributed to lower rates of negative explorations. If an aspiration event is not witnessed, misleading symptoms may delay the correct diagnosis and exacerbate the morbidity.
Pan et al reported that FBA patients under the age of 1 year are typically sent to the hospital and receive treatment rapidly after aspiration, frequently within 24 hours. 3 Two factors likely contribute to this phenomenon. First, a higher proportion of infants have a definite history (witnessed aspiration) of FBA than do older children. A second reason for rapid treatment in infants is related to the symptoms of FBA. 3 Although coughing is the predominant symptom for the majority of older children, wheezing/stridor, excessive crying, seizures, and loss of consciousness are more likely to occur among infants, which could garner more attention from parents. Foreign body inhalation should be suspected from a witnessed choking episode. Choking episodes/coughing spells have been reported to have a sensitivity of 80% to 82% and a specificity of 34% for FBA. 12 Similarly, a witnessed choking crisis has been cited as the sole clinical feature with a high sensitivity (75.4%) and specificity (92.1%) in establishing a diagnosis of FBA. 13
All the infants in the current study underwent chest X-rays. For about half of them, the X-rays were normal with no suspicious findings. In the remaining tests, one side consolidation was often seen. Authors generally distinguish between acute findings, which commonly include hyperinflation in the chest X-ray, and between later findings, which include pneumonia and atelectasis. 4 In the older group of the current study, the X-ray was normal in only 20% of the patients. This data emphasize the importance of awareness to witnessed events for the diagnosis of FBA in infants.
In our cohort, the type or origin of the FB was not associated with the length of hospitalization. In contrast, a retrospective study of 77 cases of FBA revealed shorter hospitalization, less than 10 days, following aspiration of nonorganic materials or plants other than peanuts, compared to longer hospitalization when the FB was peanuts or animal material. 13 Another study linked the type of FB to the rate of complications related to the removal of the FB. 14
Management of infants at our center included rigid bronchoscopy for FB removal under general anesthesia. The bronchoscope used was very small, the size of 3 to 3.5 (Karl Storz). The use in infants of small bronchoscopes makes the extraction of FBs more difficult, resulting in partial extraction, with retained FB in the bronchus or lungs. It also restricts the ventilation time to the lungs and prevents the use of optic setup. All these factors make the procedure more challenging for this age-group. Flexible bronchoscopy was used in 33% of the cases. The FBs were retrieved with grasping forceps.
In infants, the use of optical forceps without rigid bronchoscope is still questionable. 15 For this technique, the risk with the greatest potential is laryngospasm; the younger the infant, the greater the risk. 15
Conclusions
Foreign body aspiration was shown to be not uncommon in infants under 1 year; this group comprised 16% of FBA cases of all children at our center. A witnessed aspiration event has a high positive predictive value for FB presence. High index of suspicion is needed to rule out FBA. In light of the findings of this study, a large-scale national population-based investigation should be conducted to identify sociodemographic factors that may be associated with the incidence of FBA, and education programs at well-baby clinics should be implemented to raise the awareness of caregivers to appropriate feeding habits.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.