
Abstract
We report 2 cases of stapes surgery failure due to the depth marker groove of the piston of a Big Easy titanium prosthesis getting caught at the edge of the stapedotomy hole. In the first case, the stapedotomy failure, detected peroperatively, was corrected by modifying the angulation of the shaft of the prosthesis. In the second case, the failure occurred after a delay during which scar tissue developed around the depth marker groove, hampering the movement of the prosthesis. The usual postoperative imaging did not detect this complication. The diagnosis was made during revision surgery and the condition was treated by enlarging the hole in the footplate. Alternatively, the use of a piston without a depth marker groove would have resolved the problem. Although a rare event, the possibility of stapes surgery failure due to the depth marker groove should not be overlooked.
Introduction
The most common cause of relapsed conductive hearing loss (CHL) after stapes surgery is the dislocation of the prosthesis. 1 –3 Other reported causes are erosion of the incus, malleus fixation, periprosthetic fibrosis, and otosclerosis regrowth. 1 –3 We recently observed 2 cases of stapes surgery failure related to the design of the prosthesis. The problem was due to the depth marker groove of the piston getting caught at the edge of the stapedotomy hole. The 2 cases reported here illustrate this rare incident.
Case 1
A 38-year-old woman with unilateral otosclerosis underwent a right stapedotomy via a transcanal approach. The procedure consisted in laser-cutting a hole 0.7 mm in diameter in the footplate and inserting a Big Easy titanium piston with a shaft diameter of 0.5 mm and a length of 4.5 mm. The loop of the prosthesis was crimped to the incus sufficiently firmly to create a stable linkage. The handle of the malleus was gently raised keeping the motion of the prosthesis under observation. While testing for friction between the shaft and the stapedotomy hole, the depth marker groove of the piston got caught at the edge of the anterior margin of the fenestra. The angle of the prosthesis was then adjusted by bending the shaft with a right angle hook to obtain the optimal orientation within the fenestra. The testing manoeuver was repeated to ensure smooth movement of the piston. Hearing improved postoperatively with closure of the air-bone gap (ABG) to within 10 dB.
Case 2
A 63-year-old woman consulted at our department for a rapidly progressing right hearing loss. She had undergone a right stapedotomy a year earlier for otosclerosis. The procedure had consisted in cutting a hole 0.6 mm in diameter in the footplate and inserting a Big Easy titanium piston with a shaft diameter of 0.5 mm and a length of 4.5 mm. The piston had slid easily through the stapedotomy hole after the loop had been crimped. The immediate postoperative course was uneventful with an ABG closure to within 10 dB at the 3-month postoperative visit. At the 1 year postoperative visit, she reported a decline of her hearing over the preceding few weeks, with no dizziness or vertigo. The otoscopy examination was normal. The hearing test revealed the recurrence of CHL with an ABG of 40 dB. Multislice computer tomography (MSCT) and cone beam computer tomography (CBCT) scans did not reveal the cause of the CHL (Figure 1). The middle ear appeared well aerated, with the prosthesis correctly located, and no cause of CHL, such as malleus fixation or superior semicircular canal dehiscence, was found. An exploratory tympanotomy was performed under general anesthesia. As shown by computer tomography (CT) imaging, the prosthesis was found effectively attached to the long process of the incus with the tip of the prosthesis correctly positioned through the hole in the footplate (Figure 2). Palpation of the piston showed that it did not slide freely through the hole because the depth marker groove was caught at the edge of the fenestra. After cautiously removing the piston, we increased the diameter of the stapedotomy hole to 0.8 mm, reinserted the Big Easy piston with a shaft diameter of 0.5 mm, and sealed the oval window with small pieces of fatty tissue. Hearing improved postoperatively with closure of the ABG to within 10 dB.
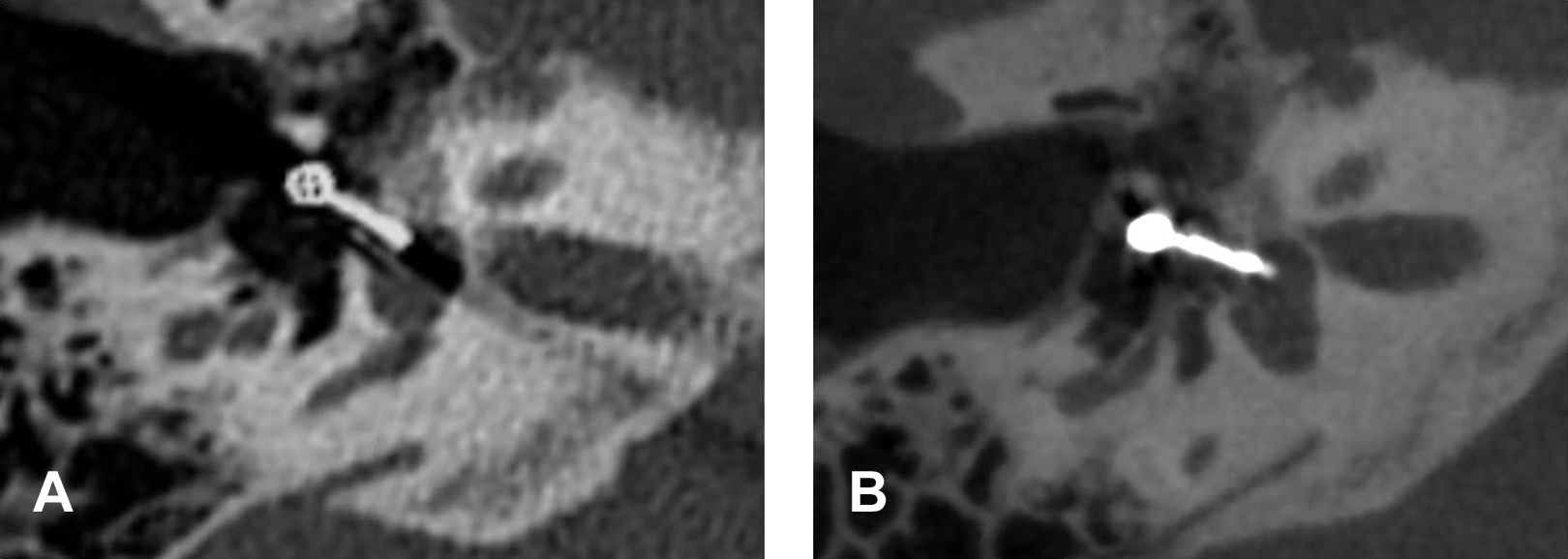
Despite metallic artefacts, MSCT (A) and CBCT (B) showed a well-located prosthesis. CBCT indicates cone beam computer tomography; MSCT, multislice computer tomography.
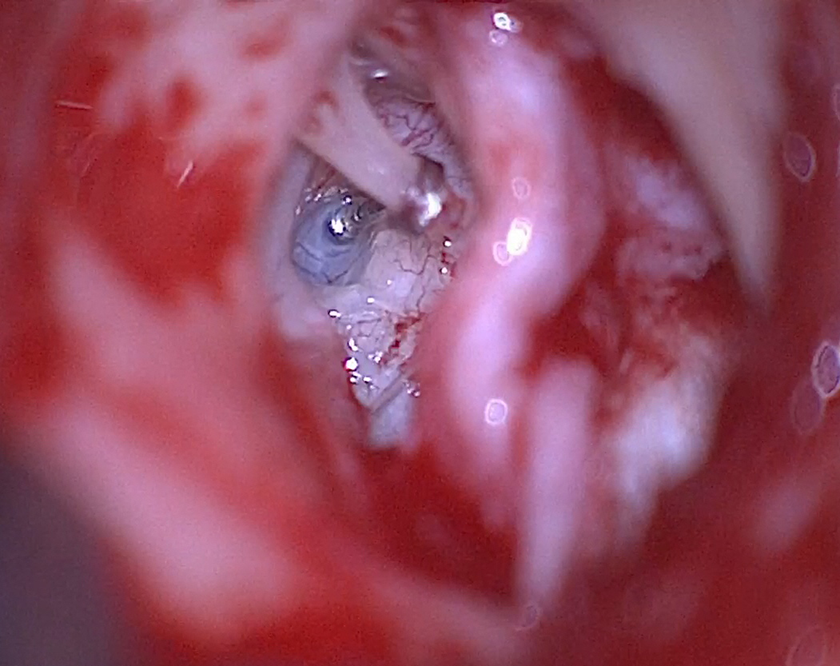
Operative view. The shaft of the piston is well positioned in the stapedotomy hole and correctly crimped around the long process of the incus without erosion.
Discussion
At the end of a stapes procedure for otosclerosis, the mobility of the prosthesis should be carefully checked. After insertion of the prosthesis in the stapedotomy hole, the crimping of the loop to the incus might slightly alter the orientation of the shaft of the piston. Inadequate angulation of the piston would be likely to lead to friction between the shaft and the margin of the fenestra. 4 With a piston without a depth marker groove, the slight modification of the orientation of the shaft would not hamper its motion through the hole in the footplate. However, with the Big Easy prosthesis, the depth marker groove may get caught at the edge of the stapedotomy hole, thus limiting the mobility of the piston. In case 1, the testing maneuver showed the depth marker groove of the piston engaged with the anterior edge of the stapedotomy hole. This led us to adjust the angle of the prosthesis to ensure smooth motion through the hole. This example highlights the importance of careful testing of the mobility of the prosthesis at the end of the procedure.
The failure of stapes surgery may also occur after a delay following the procedure. This situation is characterized by the reappearance of CHL after surgery, as has been observed in 8.6% 1 to 10.5% 2 of cases. The results of MSCT scans, routinely performed in these cases, are usually well correlated with the surgical findings. 5 –8 Most failures of the stapes procedure are due to the dislocation of the piston and the erosion or necrosis of the long process of the incus. 1,3,5,7,9 Among other causes, the prosthesis may be too short or not crimped tightly enough around the incus, 10 the movement of the prosthesis may be hampered by a narrow stapedotomy, or the development of periprosthetic fibrosis or otosclerosis regrowth. 7 Associated anomalies, such as superior semicircular canal dehiscence, round window atresia, or attical fixation, are usually detected if the imaging is done before the primary procedure, or intraoperatively, except in the case of dehiscence. 6
Sometimes the CT scan does not offer an explanation of the failure of stapes surgery, especially if the piston is blocked at the oval window. Thus, in case 2, the postoperative MSCT and CBCT scans showed the piston well located in the stapedotomy hole and correctly connected to the incus. Only surgical exploration could have detected the cause of the failure. The patient had initially undergone a platinotomy 0.6 mm in diameter with insertion of the 0.5-mm-diameter Big Easy titanium piston. The mobility of the piston, tested at the end of the procedure, had been found satisfactory. Hearing dramatically improved in the postoperative period, but decreased after 1 year.
During revision surgery, the piston was found to be prevented from sliding through the platinotomy hole because membranous tissue had invaded the depth marker groove (Figure 3). This anomaly was too subtle to be visualized on MSCT or CBCT scans. The problem was resolved by increasing the diameter of the hole from 0.6 mm to 0.8 mm. Thus, as a preventive measure, it would seem advisable to cut the hole 0.2 or 0.3 mm wider than the shaft instead of just 0.1 mm wider as we had initially done. Alternatively, the complication could be avoided using a prosthesis without a depth marker groove.
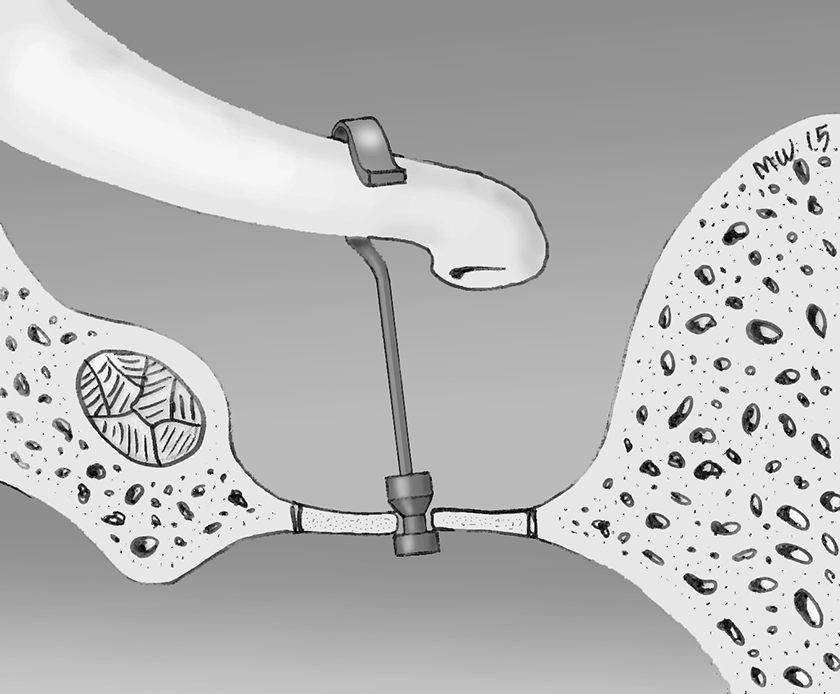
Inside view. Left ear. The piston is well connected to the incus but engaged by the edge of the fenestra at the level of the depth marker groove. (Credit: Illustration by Marc Williams).
To our knowledge, the type of failure of stapes surgery that we have recently encountered in 2 tertiary care centers has not been previously reported. Surgeons should not overlook the eventuality of this rare complication, which may escape diagnosis by the usual MSCT or CBCT scans.
Footnotes
Authors’ Note
Informed consent was obtained from all participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.