
Abstract
The aim of this prospective study was to analyze the voice and quality-of-life outcomes of microscopic diode laser surgery (MDLS). The study was conducted on a series of 46 patients with Tis–T1a glottic carcinoma treated with microscopic endolaryngeal diode laser surgery. Patients were asked to complete the Voice Handicap Index and quality-of-life questionnaires of the European Organization for Research and Treatment of Cancer. When comparing the pre- and postoperative scores, there were significant difference on the physical scores (P = .014) of the patients who underwent type III cordectomy and functional (P = .022), emotional (P = .002), and overall scores (P = .005) of the patients who underwent type IV cordectomy, in the direction of better quality of voice after MDLS. The postoperative functional, physical, emotional, and overall scores of groups were significantly increased with the extension of resection.
Introduction
The glottic cancer has major effects on basic laryngeal functions such as voice and breathing. Additionally, treatment options also have certain impacts on these functions. Nevertheless, not only the survival, the quality of voice and quality of life (QOL) of the patients are important factors while considering the treatment options.
Several outcome measures are available to assess the functional results of endolaryngeal surgery for glottic cancer. The Voice Handicap Index (VHI) is a widely used patient perceptual questionnaire that assesses the handicapping effects of a voice problem on an individual’s life. 1 Voice problems cause a substantial impact on an individual’s QOL. Quality-of-life analysis is the subjective expression of the patient about his or her own situation and relations with the others in the light of his or her ability of self-perception and assessment. The European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire–Core Questionnaire module (QLQ-C30) is the cancer-specific questionnaire that assesses the QOL of patients with cancer, and EORTC Quality of Life Head and Neck module (QLQ-H&N35) is the head and neck cancer–specific questionnaire. The QLQ-H&N35, in conjunction with the QLQ-C30, was reported as reliable, valid, and applicable to broad multicultural samples of patients with head and neck cancer. 2 The VHI, QLQ-C30, and QLQ-H&N35 questionnaires are the commonly used questionnaires to analyze the effect of a treatment modality on patients’ voice and life for glottic cancer in Turkey.
There are several types of lasers that can be used for endolaryngeal laser surgery. The 980-nm diode laser is one of those lasers. Our previous studies support that diode laser surgery is a safe and efficacious treatment modality for glottic cancer. 3,4 The estimated 3-year disease-free survival we observed was 93.1% for T1-T2 glottic tumors. 4 Despite these reports, several factors impede the standardization of treatment with diode laser. When compared with CO2 laser, it has a low wavelength that gradually increases the penetration depth. There are no reports in the literature about the effect of diode laser on quality of voice and consequently QOL for early glottic cancer. The aim of this study was to assess the effect of microscopic endolaryngeal diode laser surgery (MDLS) on voice and QOL for Tis and T1a glottic cancer.
Patients and Methods
The study involved 46 patients with Tis–T1a glottic cancer treated with MDLS at Ankara Oncology Education and Research Hospital from 2012 to 2015. The study was a prospective institutional review board–approved clinical study and the cohort was followed prospectively. All tumors were accurately visualized through an operative microscope under general anesthesia before the initial treatment, and histological confirmation of malignancy was provided. All tumors were squamous cell carcinoma. Exclusion criteria included incomplete visualization or resection of the tumor under rigid laryngoscope, history of laryngeal or major head and neck surgery, and previous voice disorder. The tumors were defined according to the 2010 American Joint Committee on Cancer–International Union against Cancer TNM system. Cordectomies were graded according to the classification of the European Laryngological Society 5 as follows: type I, subepithelial; type II, subligamental; type III, transmuscular; type IV, total; type Va, encompassing the contralateral vocal fold and the anterior commissure; type Vb, including the arytenoids; type Vc, including the ventricle; and type Vd, encompassing the subglottis.
Patients were divided into 3 groups according to extent of the resection. Group 1 consisted of patients who underwent types I and II cordectomies, group 2 consisted of patients who underwent type III cordectomy, and group 3 involved patients who underwent type IV cordectomy. Patients were asked to complete the VHI questionnaire preoperatively and 6 months postoperatively and EORTC QLQ-C30 and QLQ-H&N35 modules 6 months postoperatively. The study was approved by the institutional review board of Ankara Oncology Education and Research Hospital, and written informed consent was obtained from all patients. No identifying information was collected.
Technique
A gallium-aluminum-arsenide diode laser (Wuhan Gigaa Optronics Technology, Wuhan, China) with the following specifications was used to excise the tumor in all cases: power 3 to 6 W and wavelength 980 nm, with a 400-mm fiber and continuous wave mode. Microscopic diode laser surgery is performed through a laryngoscope with the benefit of an operating microscope. The cutting is performed with a hand-held fiber delivery system using straight or 30° angled instruments. The instruments are specifically designed for laryngeal surgery with different lengths. En block resection was preferred by cutting around the tumor and removing it in one piece.
Voice Handicap Index
The VHI is a validated questionnaire measuring psychosocial handicapping effects of voice disorders. 1 The VHI contains 30 questions concerning how voice influences patients’ lives and has been divided into 3 subscales: functional, physical, and emotional domains. Each answer is rated from 0 to 4, with 0 being normal and 4 representing the worst alternative. The total score of the 30 questions ranges from 0 to 120. Based on the final score, the quality of voice is graded. The VHI overall score is categorized as a minimal amount of handicap when the score is from 0 to 30, a moderate amount of handicap with a score between 31 and 60, and a serious amount of handicap when the score is between 61 and 120. 1 We compared preoperative and postoperative (6 months after MDLS) VHI scores within each group and postoperative VHI scores among the 3 groups. The validity of the Turkish version of the VHI was proved by the previous literature. 6
Quality-of-Life Questionnaire
The QLQ-C30 questionnaire comprises 6 functional scales (physical, social, emotional, cognitive, role, and general status), 3 symptom scales (fatigue, pain, and nausea and vomiting), and 6 independent items (dyspnea, insomnia, appetite, constipation, diarrhea, and financial difficulties). The QOL-H&N35 is the head and neck cancer–specific questionnaire that comprises 7 symptom scales (pain, swallowing, senses, speech, social eating, social contact, and sexuality) and 11 independent items (teeth, opening mouth, dry mouth, thick saliva, cough, feeling ill, pain killers, nutritional supplements, feeding probe, weight gain, and weight loss). Each scale and item is scored 0 to 100 after linear transformation. The functional scale scores are inverse: The higher the score, the better the function; but on the symptom scales and independent items, the higher the score, the greater the difficulties or symptoms. We compared QLQ-C30 and QOL-H&N35 scores 6 months after MDLS among the 3 groups. The validity of the Turkish version of the QLQ-C30 was proved by the previous literature. 7 The Turkish version of QOL-H&N35 is a widely used questionnaire for many years, but we couldn’t find any literature regarding the validity of its Turkish version. 8
Statistical analysis
The results were given as arithmetic mean (standard deviation). The Wilcoxon signed rank test was performed to analyze the difference between preoperative versus postoperative VHI scores. Kruskal-Wallis test was used to analyze the mean differences of VHI and EORTC scores between the 3 groups of patients. A significance level of P <.05 for all testing was used. The data were collected using an Excel (Microsoft, Redmond, Washington) spreadsheet. All analyses were performed by SPSS for Windows, version 15.0 (SPSS Inc, an IBM Company, Chicago, Illinois).
Results
Permanent pathologic sections revealed that all the tumors were squamous cell carcinomas, 15 Tis and 31 T1a. All glottic carcinomas were completely removed and all the patients healed without complications. There were 13 patients in group 1, 16 patients in group 2, and 17 patients in group 3, with a mean age of 58 (range, 42-68).
Voice Handicap Index
The mean (standard deviations) of preoperative and postoperative VHI overall scores of all the patients were 52.6 (25.1) and 45 (15.3), respectively. When comparing preoperative and postoperative scores of all patients, the differences were significant on all the scores, indicating a better quality of voice after MDLS (Table 1). Table 2 shows the preoperative and postoperative VHI scores of the patients according to groups. There was significant difference on the physical scores (P = .014) of the patients in group 2 and functional (P = .022), emotional (P = .002), and overall scores (P = .005) of the patients in group 3, in the direction of better quality of voice after MDLS. The postoperative functional, physical, emotional, and overall scores of groups were significantly increased with the extension of resection. Types I and II cordectomies resulted in minimal amount of voice handicap, whereas types III and IV cordectomies caused moderate amount of handicap.
VHI Scores of All Patients Before and After Diode Laser Cordectomy.
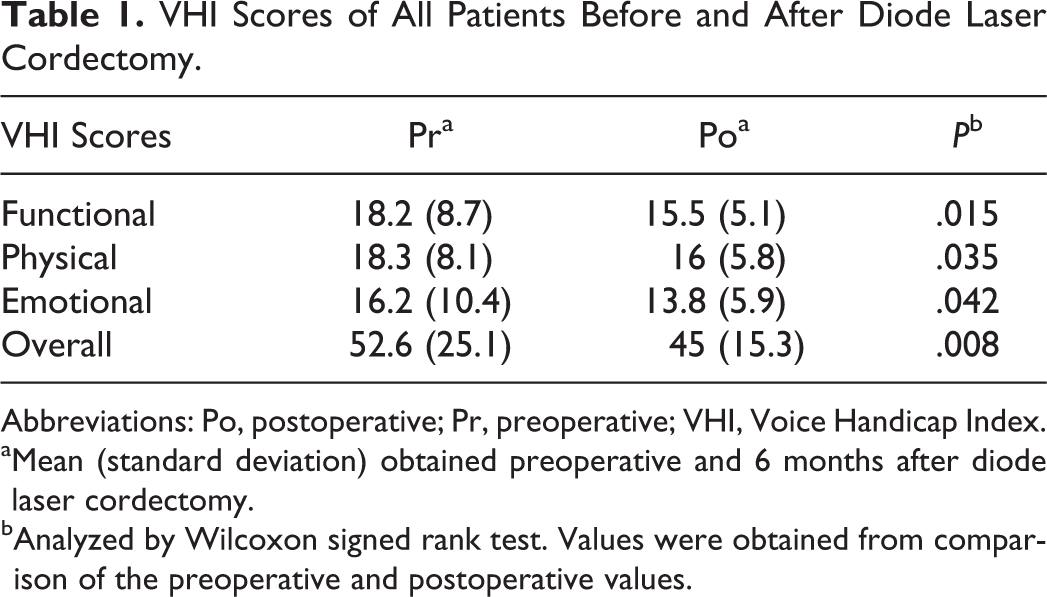
Abbreviations: Po, postoperative; Pr, preoperative; VHI, Voice Handicap Index.
aMean (standard deviation) obtained preoperative and 6 months after diode laser cordectomy.
bAnalyzed by Wilcoxon signed rank test. Values were obtained from comparison of the preoperative and postoperative values.
Voice Handicap Index Scores of Groups Before and After Diode Laser Cordectomy.
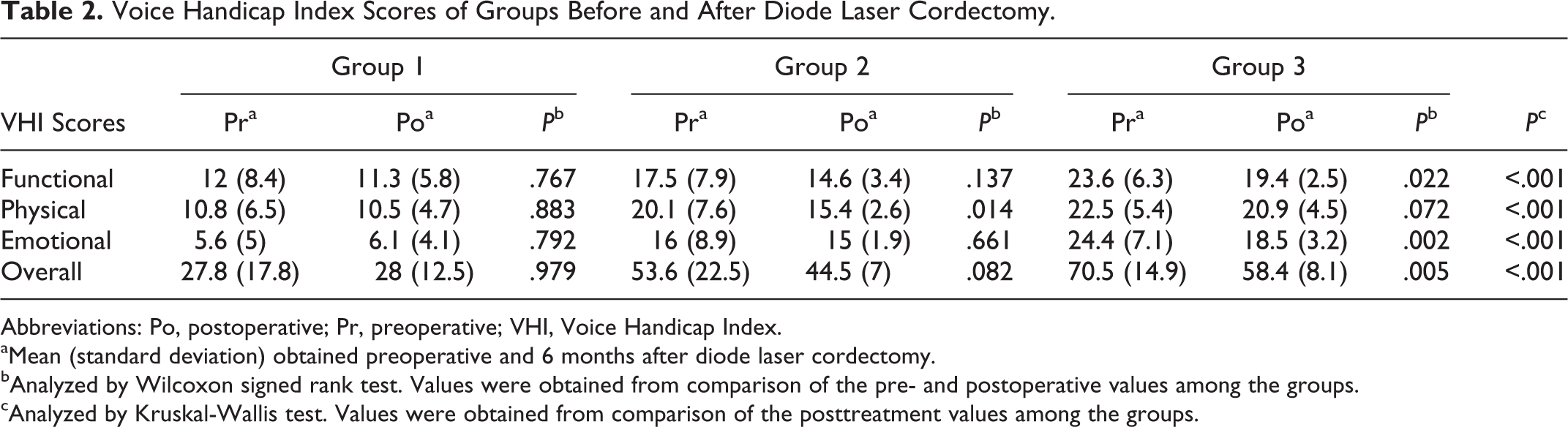
Abbreviations: Po, postoperative; Pr, preoperative; VHI, Voice Handicap Index.
aMean (standard deviation) obtained preoperative and 6 months after diode laser cordectomy.
bAnalyzed by Wilcoxon signed rank test. Values were obtained from comparison of the pre- and postoperative values among the groups.
cAnalyzed by Kruskal-Wallis test. Values were obtained from comparison of the posttreatment values among the groups.
Quality of Life
On the QLQ-C30 questionnaire, the mean values of functional scales ranged between 68 and 100, the mean values of symptom scales ranged from 0 to 18.7, and the mean values of independent items ranged from 0 to 24.9. When comparing cordectomy types, the differences between groups were significant on the general health status (P = .049), cognitive status (P = .021), and social status (P = .023) on functional scales with greater severity in group 3. The means and standard deviations of each scale are given in Table 3.
EORTC QLQ-C30 Scores After Diode Laser Cordectomy.
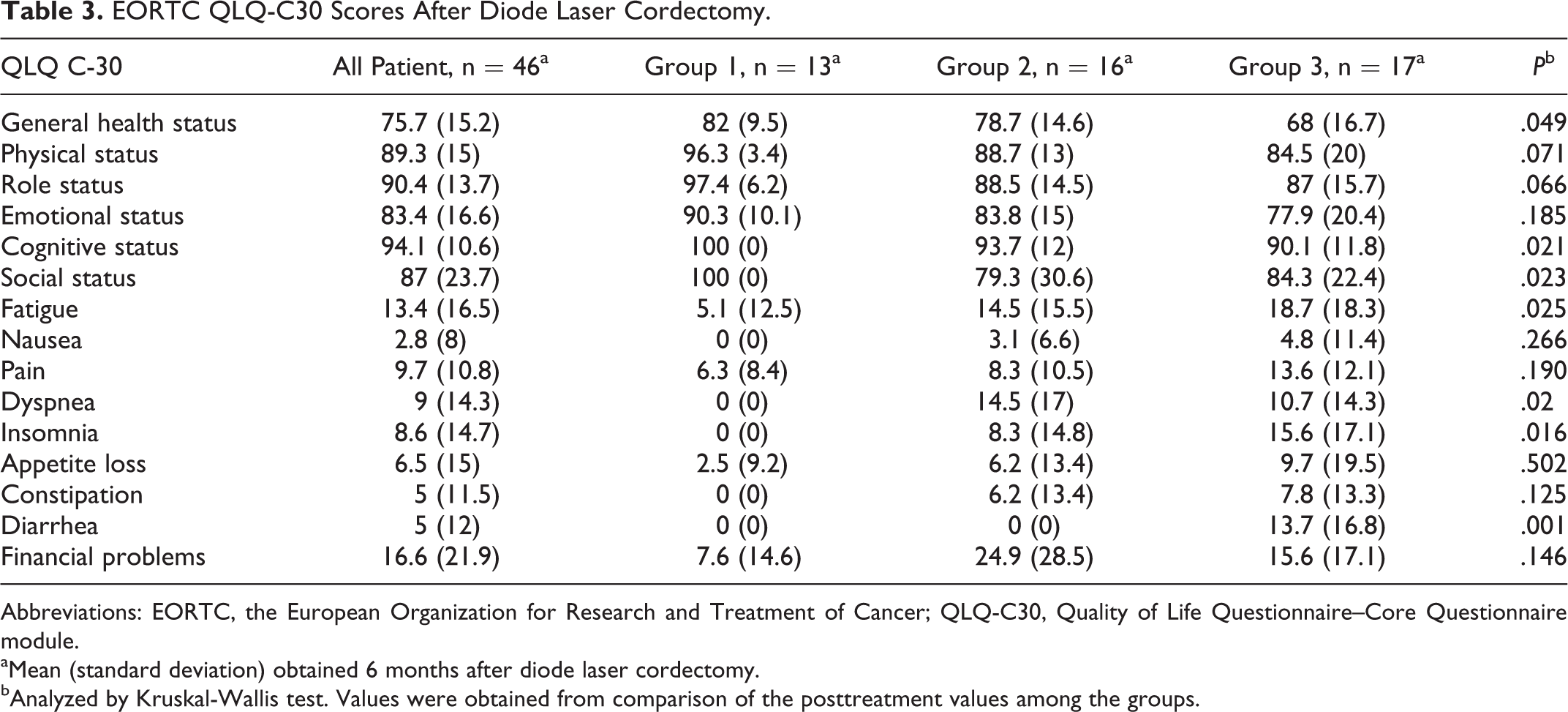
Abbreviations: EORTC, the European Organization for Research and Treatment of Cancer; QLQ-C30, Quality of Life Questionnaire–Core Questionnaire module.
aMean (standard deviation) obtained 6 months after diode laser cordectomy.
bAnalyzed by Kruskal-Wallis test. Values were obtained from comparison of the posttreatment values among the groups.
On the QLQ-H&N35 questionnaire, the mean values of symptom scales ranged from 0 to 41.1 and the mean values of independent items ranged from 0 to 37.5. Responses on the QLQ-H&N35 questionnaire showed significant differences on the pain (P = .048), swallowing problems (P = .001), senses (P = .002), social eating (P = .008), and social contact (P = .005) on symptom scales with greater severity in group 3. The means and standard deviations of each scale are given in Table 4.
EORTC QLQ-H&N35 Scores After Diode Laser Cordectomy.
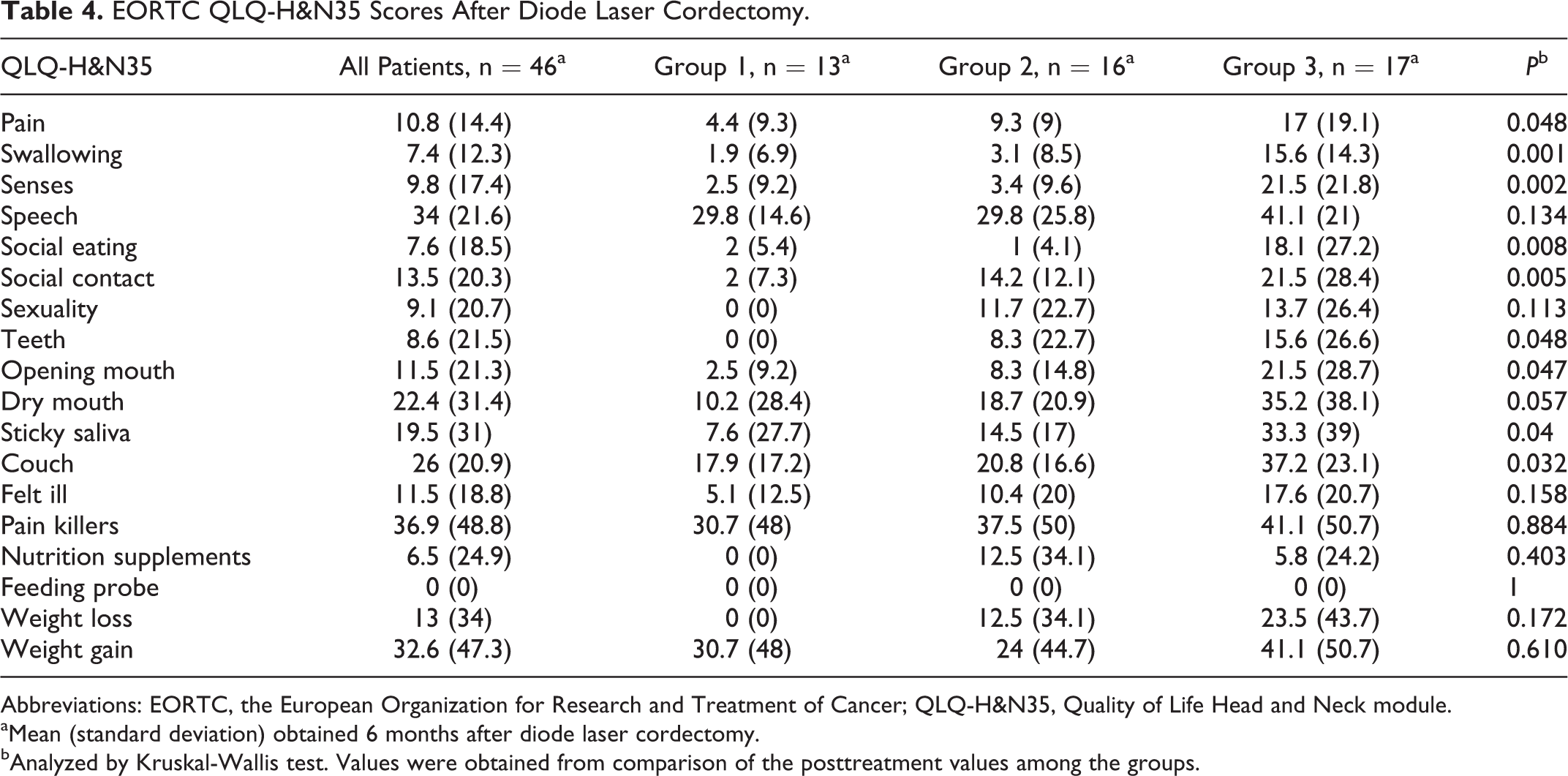
Abbreviations: EORTC, the European Organization for Research and Treatment of Cancer; QLQ-H&N35, Quality of Life Head and Neck module.
aMean (standard deviation) obtained 6 months after diode laser cordectomy.
bAnalyzed by Kruskal-Wallis test. Values were obtained from comparison of the posttreatment values among the groups.
Discussion
The degree to which a voice disorder impacts a patient’s functional, physical, emotional, and social well-being is highly variable and based on many factors unique to the individual. 9 Evaluating the impact of a voice change on the patient’s overall QOL may determine the course of treatment. Voice change is the major complain and fear of the patients with early glottic cancer. The goal of the treatment is to preserve the quality of voice with best oncologic outcomes. The 2 major choices of treatment, including endolaryngeal CO2 laser microsurgery and radiotherapy, provide similar 5-year disease-specific survival rates for early glottic cancer. 10,11 When considering voice, VHI scores were comparable following transoral CO2 laser microsurgery and radiotherapy in the current literature, suggesting no clinically significant difference in functional voice outcomes between treatment types. 12 Additionally, better VHI outcomes were reported following lower (types I and II) versus higher types of resections (type III). 12
The oncologic results of diode laser are comparable with CO2 laser and radiotherapy. 4 Although there are numerous studies about the impacts of endolaryngeal CO2 laser microsurgery and radiotherapy on voice and QOL, this is the first report analyzing the impact of MDLS on voice and QOL. We used patient-based questionnaires to determine the psychosocial handicapping effects of the MDLS on patients with Tis and T1a glottic cancer.
The descriptive results of this study with regard to VHI were not so similar to those previously reported in the literature for CO2 laser surgery and radiotherapy. Most of the preoperative and postoperative VHI scores of our patients were higher than those who had early glottic tumors and underwent CO2 laser surgery or radiotherapy in the literature. 13 -16 The difference in preoperative VHI scores can be a result of cultural factors as well as relatively younger age of our patients. The high preoperative scores have a major effect on the high postoperative scores. But on the other hand, the high postoperative scores may indicate that MDLS has greater impact on voice quality than CO2 laser and radiotherapy. Previous reports represent a statistically significant improvement on the VHI scores after radiotherapy. 15 Likewise, when comparing preoperative and postoperative scores, the differences were significant on all the VHI scores, indicating a better quality of voice after MDLS. The overall VHI scores of all the patients showed a moderate handicap.
With the idea that more extensive vocal fold resections would be thought to worsen voice, we analyzed the effect of cordectomy types on VHI and QOL scores. The results of VHI scores supported this correlation, whereas only a few parameters in QOL scores showed significant difference. When comparing the preoperative and postoperative scores among cordectomy types, there was significant difference on the physical scores of the patients who underwent type III cordectomy and the functional, emotional, and overall scores of the patients who underwent type IV cordectomy, in the direction of better quality of voice after MDLS. Comparisons of the VHI scores between types of cordectomies after MDLS showed that the lowest voice handicap was seen in types I and II cordectomies and the highest voice handicap was seen in type IV cordectomy. Types I and II cordectomies resulted in minimal amount of voice handicap, whereas types III and IV cordectomies caused moderate amount of voice handicap.
The QLQ-H&N35 scores of CO2 laser with regard to cordectomy types demonstrated a significant difference only in the speech and social contact scores with greater severity in the type V cordectomy and anterior commissure resection. 13 The present study identified significant differences on the pain, swallowing problems, senses, social eating, and social contact on symptom scales with greater severity in the type IV cordectomy group. Consequently, previous studies showed that some of the scales from QLQ-H&N35 and QLQ-C30 modules could be influenced by patient characteristics. 17 The EORTC QLQ questionnaires are specifically developed for use in international trials and they facilitate comparisons across studies. 17 They assess relatively different dimensions of QOL. This report presents the basic results of these modules after MDLS.
The time required for the voice quality to achieve a stable condition after laser surgery is still not clear. It has been shown that the voice quality of patients with early glottic cancer who underwent transoral laser surgery can achieve a stable status at 6 months after surgery, so we analyze the outcomes at 6 months after MDLS. 18 A limitation of the present study may lay in the lack of acoustic analysis. That is because most of our patients refused to complete the postoperative analysis because the laryngology center was in another unit in the town. One of the major disadvantages of VHI is that the responses on the VHI may be affected by personal circumstances, such as social situation, employment, mood, personality, and activities of daily living. 19 These circumstances are not likely to similarly affect the results of acoustic and aerodynamic testing. Nevertheless, many studies have identified good correlations between acoustic and aerodynamic measures and the 3 subscales of the VHI (functional, emotional, and physical) for vocal fold lesions. 18 Among the limitations of this study, the sample size was small and all the patients had Tis and T1a glottic cancer. We limit our study with Tis and T1a tumors as it has been demonstrated that voice quality outcomes of laser surgery are similar or better than radiotherapy for patients with limited T1a tumors, whereas laser resection of larger tumors results in poorer outcomes. 16,20
The gold standard for transoral laser microsurgery for laryngeal cancer is the CO2 laser. The standard CO2 laser device is a straight line beam delivery system from surgical microscope causing difficulty in the management of deep and curved areas of the larynx. Special precautions are needed to avoid the damage of beam in the operating room and surgical field as the beam moves in every movement of the microscope. These drawbacks favored the application of flexible fiber-based lasers. Although the fiber-based CO2 laser has been introduced, it is more accepted for robotic surgery rather than microscopic surgery. Diode laser is a portable flexible fiber-based laser, the fiber passes through a straight or angled hand-held fiber guidance instrument that can be held and managed like a forceps, and the fiber directly contacts tissue. Many studies show that the diode laser is easily used, efficient, and safe for the management of different pathologies in the larynx. 21,22 The fiber system lets the surgeon resect deep and angled parts of the larynx easily and makes it much safer to use than standard CO2 laser. 3 It has excellent hemostatic properties as a result of high absorption by hemoglobin. 23 It is portable, small, and relatively inexpensive. The 980-nm diode laser is a new technology, and it recently has been introduced for the treatment of early glottic tumors. 3 , 4 These features of the 980-nm diode laser allow it to become a strong alternative to the CO2 laser.
Our results showed that the VHI scores became better after MDLS. Similar with CO2 laser, voice quality after MDLS is closely associated with extent of resection. Further studies are needed to analyze the acoustic and aerodynamic parameters to demonstrate certain outcomes about the impact of MDLS on quality of voice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.