
Abstract

Introduction
Necrotizing fasciitis is characterized by severe infection of the soft tissues and fascia. Involvement of the head and neck is rare but carries significant morbidity and mortality. Cervical necrotizing fasciitis (CNF) represents an aggressive form of deep neck space infection and is associated with a high-mortality rate of 40% to 76%. 1
The disease is usually polymicrobial in origin and includes mixed aerobic and anaerobic species. 2 Prompt diagnosis and treatment are necessary in the management of CNF. Although the extent of infection varies, patients with CNF are usually in critical condition and may require intubation or tracheostomy. Treatment involves intravenous antibiotics and repeated surgical debridements. 3
In most cases, multiple episodes of debridement are necessary, potentially resulting in significant soft tissue defects. After all nonviable tissue is excised and the infection is cleared, reconstruction with soft tissue flaps may be necessary, especially in patients with massive defects. We present a series of aggressive cases of CNF that resulted in massive defects, with greater than 10 cm of tissue loss in the greatest dimension.
Patients and Methods
A retrospective case series was designed to analyze patients with necrotizing fasciitis of the head and neck between 1998 and 2016 treated by the 2 senior-most authors in a tertiary care setting. The study was approved by the institutional review board of John Peter Smith Hospital (Fort Worth, Texas). Massive CNF was defined by a final defect size greater than 10 cm in the largest linear dimension. Patients with smaller defects were excluded from the study. The initial diagnosis of CNF was made according to clinical presentation, which may involve rapid progression of edema, discoloration, erythema, disproportionate pain, crepitus, tachycardia, hypotension, sepsis, and based on identification of gas within imaging of the neck. 4 Surgical findings of necrotic tissue confirmed the diagnosis in all cases. Sepsis was defined as meeting 2 or more criteria of systemic inflammatory response syndrome (temperature > 38 C or < 36 C, heart rate of > 90/min, respiratory rate > 20/min or PaCO2 < 32 mm Hg, white blood cell count >12 000/mm3 or < 4000/mm3 or > 10% immature bands) concurrent with the identification of an infectious source.
Variables analyzed included age, sex, microbiology, presence of an immunocompromised state, number of debridement, time to final surgery in days, need for tracheostomy, type of surgical reconstruction, and survival.
Results
Ten consecutive patients met the criteria for the study, including 5 males and 5 females. The characteristics of each patient are outlined in Table 1.
Characteristics of Patients.

Abbreviations: CDP, cervico-delto-pectoral flap; COPD, chronic obstructive pulmonary disease; GAS, group A streptococcus; OR, operating room; RAFF, Rectus abdominis free flap; RFF, radial forearm free flap; SCAIF, supraclavicular island flap; M, male; F, female.
Patient ages ranged from 54 to 69 years with a mean of 58.7. Six of the 10 patients possessed medical comorbidities, with type 2 diabetes being the most common (4 patients). Two other patients had chronic obstructive pulmonary disease. One patient had both type 2 diabetes and lupus and was the only patient from the series who did not survive.
Clinical findings on initial presentation included cervical erythema, tenderness, respiratory distress, and sepsis. Cultures demonstrated mixed flora in most cases. Group A Streptococcus was present in the majority of patients (7 cases). Patients were initially treated with empiric, broad-spectrum, intravenous antibiotics, which were then narrowed per wound culture results.
All patients underwent multiple surgical debridements over several days to weeks. The number of debridements ranged from 2 to 9, with the average being 4.6, over a mean period of 14.5 days. Between surgical procedures, wounds in 9 patients were treated with 0.25% acetic acid solution soaked gauze packing and changed every 6 hours on a daily basis. One patient with an anterior neck wound with pharyngeal involvement was managed with a vacuum-assisted closure dressing (VAC), involving an intraluminal pharyngeal sponge combined with an external neck sponge. Acetic acid solution was applied through the VAC system twice daily.
Tracheostomy was performed in 7 of 10 patients. Pharyngeal involvement was present in 5 patients. Bony involvement was present in 3 patients, with 2 requiring mandibulectomy and 1 requiring a partial sternum and rib resection. One patient underwent orbital exenteration.
All 9 surviving patients underwent reconstructive surgery to correct the resultant defects. All major vessels of the neck, including the carotid artery, were covered with soft tissue to prevent blowout. The reconstructive techniques included local advancement flaps (1 patient), regional pedicled flaps (5 patients), and free tissue transfer (3 patients). One patient remained feeding tube dependent at 7-year follow-up. No patients remained tracheostomy dependent. For illustrative purposes, we have included images of the clinical course of the patient that required a resection of sternum and (Figures 1 –5).

A 69-year-old female with no medical comorbidities presented with bruising and anesthesia over the anterior neck skin.

Appearance of the wound after initial debridement. Large anterior cervical cutaneous defect. Fascia appears intact and viable.

Appearance of the wound after a series of 5 debridements over the course of 14 days. Defect includes several ribs, partial sternectomy, and partial pharyngectomy and laryngectomy.
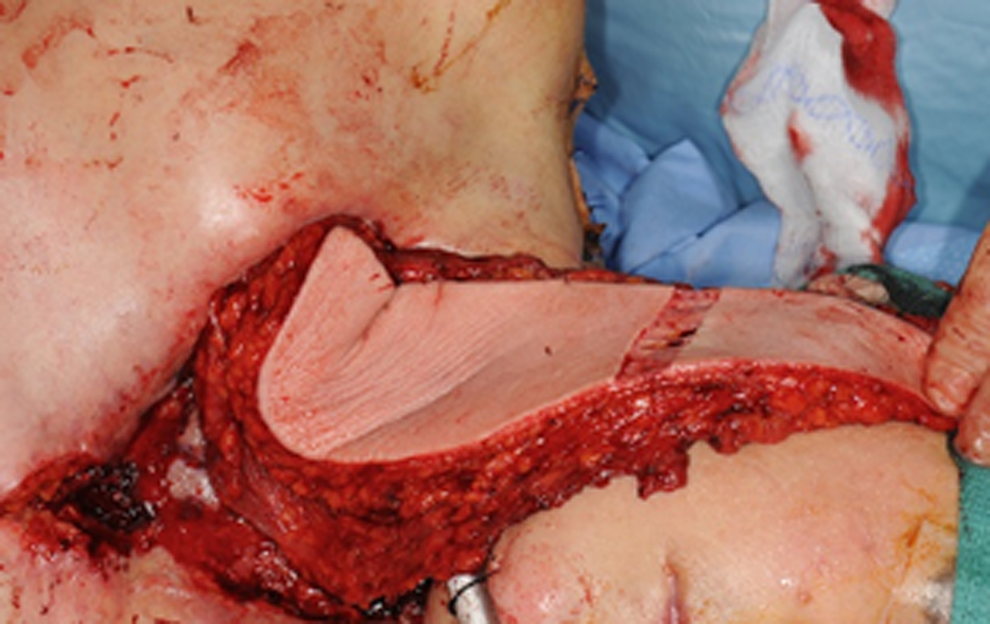
Reconstruction is performed with a latissimus dorsi flap. The flap is de-epithelialized and a portion is turned in to reconstruct the pharynx.

The flap after inset and tracheostomy.
Discussion
Cervical necrotizing fasciitis is associated with significant morbidity and mortality. The typical rapid disease progression requires aggressive medical and surgical care. Broad-spectrum, intravenous antibiotics and repeated, aggressive debridements with removal of all necrotic tissue are necessary. Airway management is critical, and the surgeon should have a low threshold for intubation and tracheostomy.
The 3 largest series to date of necrotizing fasciitis of the head and neck are those by Lin et al, Lanisnik et al, and Tung-Yiu et al. 5 -7 However, these studies are not limited to massive infections. Lin and co-authors described 47 cases over a 12-year period. On average, each patient underwent 2.6 surgical operations. Twelve patients received split-thickeness skin grafts, and 21 patients were reconstructed with local rotational or advancement flaps. The overall mortality rate was 25.5%.
Lanisnik’s group reviewed 34 cases of CNF over a 14-year period. All patients underwent debridement and were reconstructed with skin grafts. In the article by Tung-Yiu and colleagues, 11 cases of CNF of odontogenic origin are presented. Each patient underwent an average of 2 debridements, with only 2 requiring split-thickness skin grafts for wound closure.
Our series is the first to focus specifically on cases of massive CNF. Therefore, it is not surprising that our patients required more extensive surgical debridements (4.6 procedures over 14.5 days) and more complex reconstruction (10 major soft tissue flaps in 9 surviving patients) than the data in the current literature.
The microbiology observed in our case series is consistent with previously published data, with cultures demonstrating mixed flora and a high prevalence of group A Streptococcus. Furthermore, our case series shows that most of these patients are not elderly, with the average age being 58.7. Additionally, our patients were only mildly immunocompromised with 4 patients carrying the diagnosis of type 2 diabetes. One patient with the dual comorbidities of diabetes and lupus was the only patient who did not survive.
We noted a high incidence of pharyngeal involvement in cases of massive CNF, with 50% of our patients necessitating partial pharyngectomy to clear disease, and 2 of these patients requiring partial laryngeal resections. Bony involvement was observed in 4 cases, with 2 patients undergoing partial mandibulectomy, 1 needing a calvarial resection with orbital exenteration, and 1 having a resection involving sternum and rib.
The survival rate noted in our study was 90%, which was higher than the overall survival in the literature. 5 -7 Given the severe presentations and resultant significant defects, this may be reflective of more aggressive interventions and higher amount of surgical debridements, which was greater on average than other studies. 5-6 Hence, it must be stressed that a complete debridement should be performed, with removal of all concerning tissue. The authors advocate for an aggressive excision of any necrotic material, including the pharyngeal wall, larynx, cranial nerves, or bone. Necrotizing fasciitis may progress rapidly. A strategy of watchful waiting may ultimately lengthen the time to elimination of disease, lead to greater morbidity, and potentially diminish survival rates.
Wound care is critical between operative interventions in necrotizing fasciitis. As mentioned earlier, the authors generally favor 0.25% acetic acid–soaked wet-to-dry gauze packing. Repacking is required every several hours (every 2-6 hours) in order to maximize the antiseptic effect and to keep the wound clear of secretions when in communication with a tracheostomy or when pharyngeal involvement is present. In cases of anterior neck CNF where the patient is intubated, it may be advisable to delay tracheostomy until reconstruction is performed so that the wound is not in communication with the tracheal lumen.
Negative pressure wound therapy may also be utilized in cases of CNF in conjunction with antiseptic solutions such as acetic acid, which can be instilled through the VAC system in newer model machines. 8 Use of the VAC can reduce the need for frequent dressing changes, but successful application can be difficult in the head and neck region due to problems with successful seal formation. We have previously constructed a system of concurrent external and intraluminal wound VAC after a case of severe head and neck necrotizing fasciitis with successful seal and eventual healing of residual tissue, allowing us to safely reconstruct the subsequent defect. 9
Reconstruction should be undertaken once the surgeon is confident that the infection has been eliminated, and healthy granulating tissue is present in the wound bed. Standard reconstructive principles apply; however, inflammation may make vessel dissection for microvascular anastomosis more difficult. In such cases, it may be possible to find suitable donor vessels outside the neck or to utilize regional pedicled flaps. In our series, 4 free flaps and 6 pedicled flaps were utilized, without any complications.
Conclusion
Necrotizing fasciitis of the head and neck is a rare yet critical disease entity. Intensive medical and surgical care are crucial for treatment. A high index of suspicion is warranted for patients with type 2 diabetes or those taking immunosuppressive medications. Multiple surgical procedures are necessary and can result in massive defects. Even in severe cases, survival is likely when an aggressive treatment strategy is employed. The treating physician should secure the airway, aggressively debride, and proceed with reconstruction after the infection is cleared.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.