
Abstract

Case Report
A 68-year-old veteran with multiple comorbidities is referred by his primary care practitioner (PCP) for inability to clear throat mucus. The patient had quit smoking 3 years previously, consumed 3 or 4 beers per week, and denied dysphagia or weight loss. He reported that his voice had been “gruff” for years.
The patient’s problem list included type 2 diabetes mellitus, hypertension, hypercholesterolemia, coronary artery disease, 3 cardiac stents, chronic obstructive pulmonary disease, prostatic hypertrophy, gastroesophageal reflux disease (GERD) with hiatal hernia, chronic back pain, bilateral knee osteoarthritis, obstructive sleep apnea, post-traumatic stress disorder, exogenous obesity, depression, and anxiety. He denied cardiac symptoms but had limited his activity due to his obesity, back pain, and dyspnea on exertion.
He was taking 28 active medications including metformin, hydrochlorothiazide, simvastatin, and apixaban. Omeprazole in the morning and ranitidine at bedtime failed to control his GERD symptoms. He was on 2 inhalers for his chronic obstructive pulmonary disease, a steroid/bronchodilator combination and rescue albuterol. Daily cetirizine and fluticasone had failed to control his nasal symptoms. Tamsulosin and oxybutynin controlled his bladder symptoms. His depression had been managed with sertraline and alprazolam for many years, but due to recent exacerbation, amitriptyline was recently added. His chronic back pain was managed with daily cyclobenzaprine and oxycodone as needed for exacerbations.
The patient arrived in a motorized wheelchair. Physical examination revealed a large man weighing 161 kg (355 pounds) with a body mass index of 41.3. The oral examination was significant for dry mucus membranes.
Flexible nasopharyngoscopy revealed dry nasal mucosa with crusting and old blood on the septum and anterior turbinates. Strands of mucus were visualized, but no purulent sinus drainage was noted. Examination of the naso, oro, and hypopharynx revealed copious adherent yellow-white mucus with an adherent dry crust visualized in the nasopharynx (Figure 1). Mucus was also adherent to the supraglottic structures and the vocal cords, but cleared with a cued cough. Both vocal cords were mobile, mildly edematous, with bilateral pseudosulcus and postcricoid edema. There was no pooling in the pyriform sinuses and no evidence of candidiasis. A glass of water rinsed most of the mucus from the oropharynx and hypopharynx.
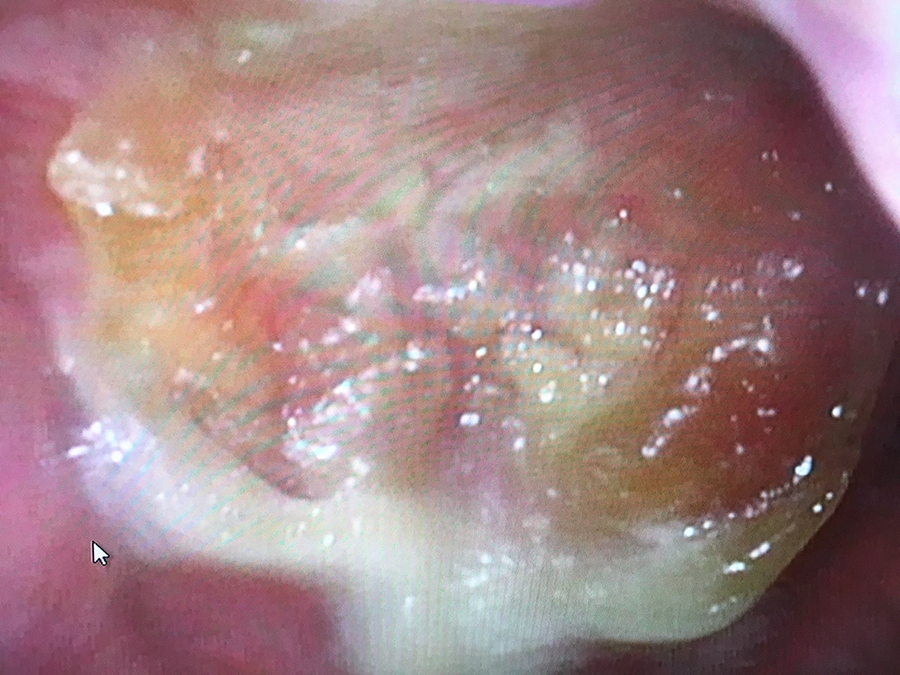
With an adherent dry crust visualized in the nasopharynx.
The patient was shown the images of his examination and counseled regarding the role of his medications leading to xerostomia and dry mucus. He was advised that it was likely not possible to eliminate most of the responsible medications but that he and his PCP should discuss whether some could be eliminated. He was told to stop the cetirizine and fluticasone, use a sterile saline nasal spray several times a day, and sip on water to help rinse the mucus from his pharynx and clear the refluxed gastric secretions from his distal esophagus.
Commentary
Polypharmacy is widely recognized as a significant impediment to well-being of older patients in developed countries. There are myriad reasons for this, some of which are listed in Table 1. Perhaps the most prominent is the “silo” effect of care provided by multiple specialists, each focusing on one physiologic system. Our patient’s symptoms were due to the combined effects of his diuretic as well as the multiple medications with anticholinergic effects.
Factors Contributing to Excess Medication Prescribing.

Geriatricians have long recognized the impact of polypharmacy (which can be defined as too many medications for this patient) in the elderly. The issue is neither new nor unknown; a recent search in PubMed yielded over 5400 citations. Specific recommendations for prescribing to the elderly, such as the Beers Criteria published by the American Geriatric Society (currently under revision), are available but not widely utilized (https://geriatricscareonline.org/ProductAbstract/2019-ags-beers-criteria-pocketcard/PC007, Accessed March 2, 2019).
The adage often articulated by geriatricians that “any symptom in an elderly person is a medication side effect until proven otherwise” should be recognized by all physicians. In this case, the otolaryngologist was the first provider to associate the patient’s complaints with his medications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.