
Abstract
Primary spontaneous cerebrospinal fluid (CSF) rhinorrhea is an unusual phenomenon that may occur anywhere along the skull base. However, CSF leaks originating from clival defects are rarely reported in the literature. The majority of reported cases were managed with microscopic techniques, using free grafts. The present study discusses a case of spontaneous CSF rhinorrhea from a clival defect closed with our transnasal operative approach using endoscopic techniques. The skull base defect was successfully managed with an endoscopic binostril approach to create a nasal septal flap pedicled at the sphenopalatine artery, while also preserving the integrity of the nasal septum.
Introduction
There are few reports on the management of clival defects using transnasal endoscopic approaches due to the rarity of spontaneous cerebrospinal fluid (CSF) rhinorrhea originating from this site. 1 Endoscopic techniques for repairing clival CSF leaks typically involves removal of the posterior nasal septum in order to allow 2 surgeons to work through both nostrils. 2,3 Other approaches have performed complete ethmoidectomies, maxillary antrostomies, and middle turbinate removal in order to create more working space for the surgeons. 1 –4
Recently, the concept of raising pedicled mucoperichondrial flaps from the nasal septum based on branches of the sphenopalatine artery has gained increasing popularity. 5 These pedicled flaps have a robust blood supply to aid with the closure of skull base defects, even at the posterior fossa. In a recently described approach, 4 removal of other nasal structures for the creation of the nasal septal flap was not required for adequate exposure and could potentially decrease the morbidity of the procedure.
We present a rare case of spontaneous CSF leak originating from a defect in the clivus and endoscopic closure with a nasal septal flap utilizing a binostril approach while also maintaining the integrity of the nasal septum.
Case Report
An obese, 48-year-old woman was referred to our institution with a 5-year history of rhinorrhea and headaches. She reported no history of meningitis or other medical complaints. The patient was on thyroid hormone replacement for a history of hypothyroidism. There was no history of head trauma or other medical conditions. Neurologic and head and neck examinations were normal except for clear and abundant rhinorrhea from the left nostril. On nasal endoscopy, the clear fluid was visualized with a 30° endoscope originating from the posterior aspect of the nasal cavity.
Computed tomography localized the site of the skull base defect at the middle portion of the clivus. Magnetic resonance imaging on T1-weighted sequence with gadolinium demonstrated an interruption of the sphenoid mucosal enhancement in front of the bone defect at the medial part of the clivus. There was no sign of empty sella syndrome (Figure 1).
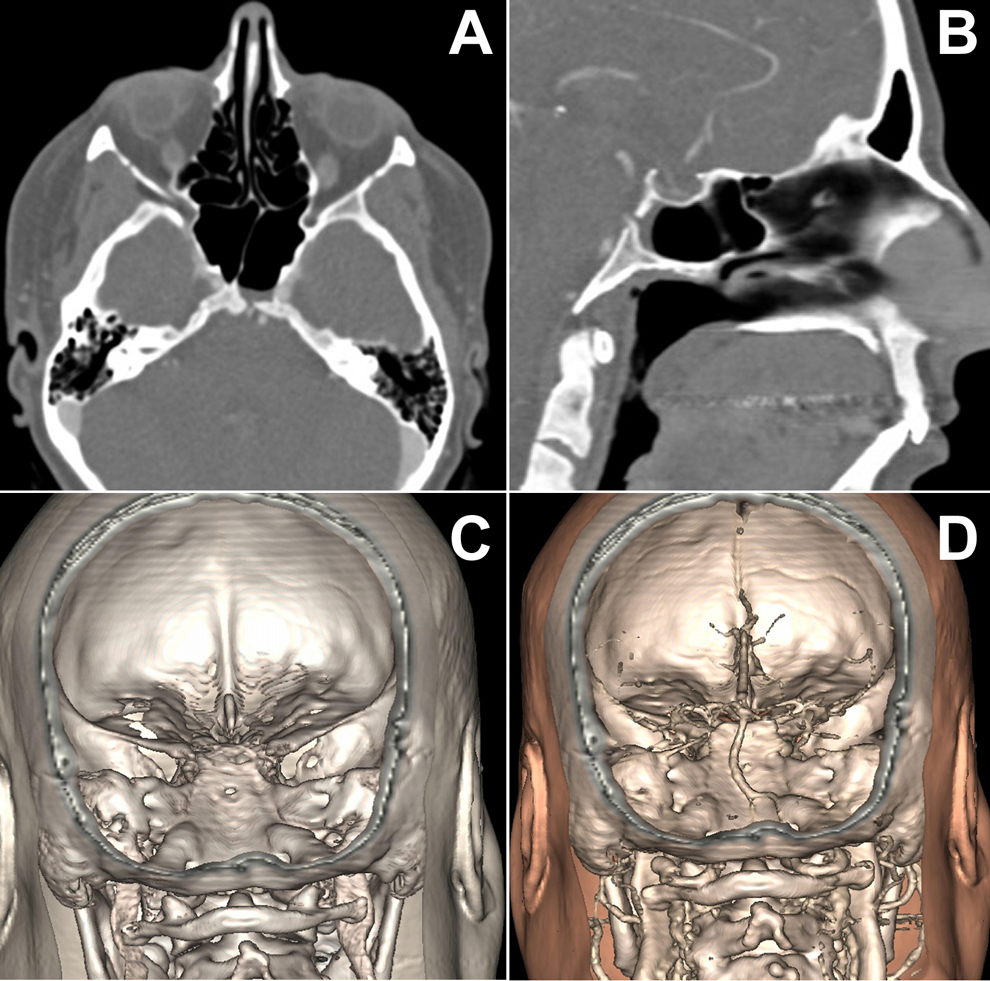
Imaging studies. A, Axial view of a computed tomography (CT) scan demonstrating a skull base bony defect at the clivus. B, Sagittal reconstruction demonstrating the same skull base defect at the clivus. C, Tridimensional reconstruction revealing the small clival defect. D, Tridimensional reconstruction of the CT showing the relationship between the clival defect and the basilar artery.
After careful preoperative evaluation, informed consent, and institutional review board’s approval (Hospital Professor Edmundo Vasconcelos, São Paulo, Brazil), the surgery was performed. After the nasal septum was infiltrated with local anesthetic with epinephrine for hemostasis, a classic anterior hemitransfixion incision for septoplasty was made on the right side. A mucoperichondrial/mucoperiosteal dissection was performed on both sides. The posterior bony septum was removed, and the sphenoid rostrum, anterior face of the sphenoid sinus, and both sphenoid natural ostia were exposed through this initial transseptal approach.
Through the left nostril, a nasal septal flap pedicled on the septal branch of the sphenopalatine artery was created with an inferior horizontal incision at the choanal arch with anterior extension and a superior horizontal incision, parallel to the first. The flap was placed into the nasopharynx creating a “septal window” on the left side. This allowed insertion of the surgical instruments. After a wide sphenoidotomy, the intersinus septum was removed and the defect was visualized in the middle clivus. The site was repaired by removing the posterior sphenoid mucosa, and the nasal septal flap was repositioned over the skull base defect (Figure 2). No free underlay or overlay grafts, such as fat, fascia lata, or cartilages, were used. Hemostatic materials were inserted over the flap to keep pressure and ensure stability. No lumbar catheter was placed.
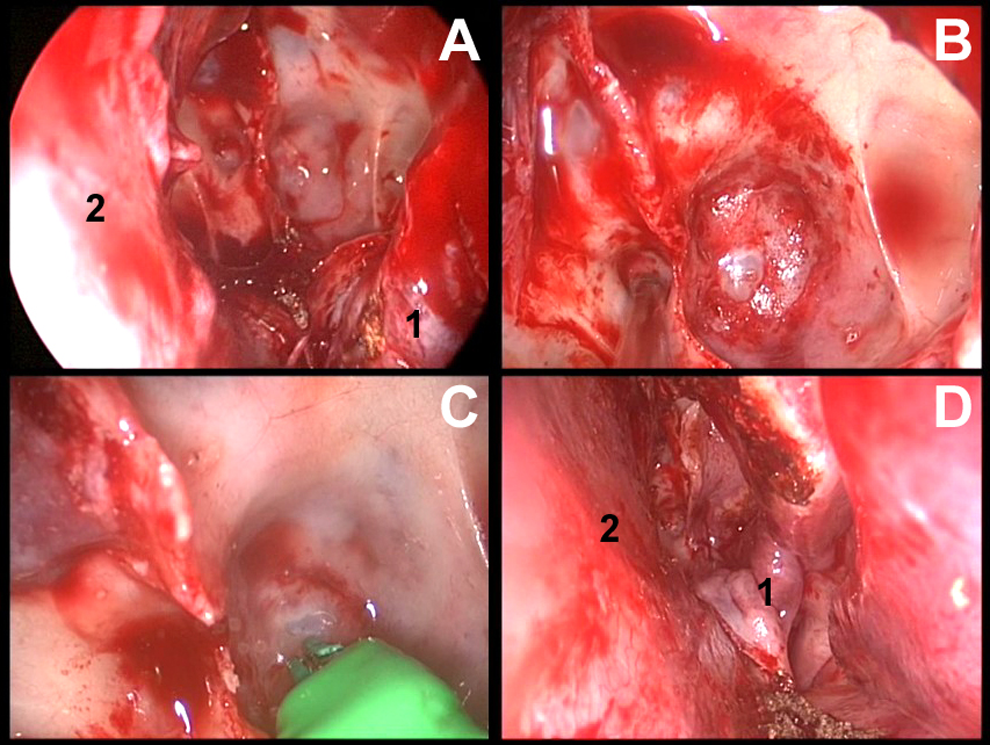
0-degree, 5-mm endoscopic view of the clival defect repair. A, Sphenoid sinus exposure after elevation of the nasal septal flap (1) creation and positioning. Note the integrity of the nasal septum (2). B, View of the defect at the middle clivus. C, Bipolar cauterization of the defect. D, Placement of the nasal septal flap (1) at the end of the procedure. The defect is completely covered with no cerebrospinal fluid (CSF) leak. The posterior septum is maintained.
Discussion
Many endoscopic approaches to sphenoid and clival CSF leaks employ complete removal of the superior posterior nasal septum, ethmoidectomies, maxillary antrostomies, and, in some cases, middle turbinate removal, in order to gain space for 2 surgeons to work through both nostrils. We utilized a recently described binostril sphenoid approach that allows excellent working space, creates a nasal septal flap, and maintains mucosal integrity on the contralateral side. As the approach is more conservative and preserves natural structures, it could provide benefit to patients postoperatively.
Conclusion
This rare case of a clival skull base defect was managed with novel binostril endoscopic techniques that allowed closure with a nasal septal flap but preserved the integrity of the nasal septum. There were no complications or CSF recurrence observed at last clinical follow-up. We will continue to monitor her for signs and symptoms of intracranial hypertension or recurrence of a CSF leak.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.