
Abstract

A 61-year-old male with schizophrenia from rural community in Bolivia presented to the emergency room at a referral hospital in La Paz, Bolivia. At presentation, he was disoriented and was unable to provide other history. Upon examination, he had a large open scalp wound of 15 × 13 cm in the mastoid-temporal area and absence of 95% of the pinna (Figure 1). Computer tomography of head revealed no bony destruction, mastoiditis, or intracranial pathology (Figure 2). Patient was initially started on intravenous antibiotics (ciprofloxacin and gentamycin which was broadened to nitrofurantoin, cefotaxime, and metronidazole) and underwent surgical debridement. Tissue specimen obtained during debridement was sent for culture and pathology review.

Clinical presentation of a 61-year-old Bolivian patient with near-complete destruction of external ear and temporal soft tissue defect from myiasis in his left head.
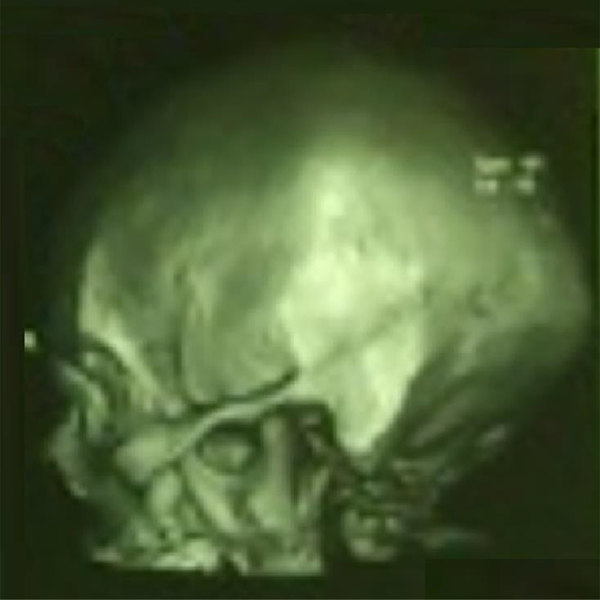
Three-dimensional reconstruction of computed tomography head of the patient demonstrating absence of bony involvement.
Tissue culture identified Ascaris lumbricoides, Trichuris trichiura, and larvae of Strongyloides stercoralis confirming the diagnosis of myiasis. Pathologic review of the specimen showed chronic inflammation and fibrosis of the external auditory canal and middle ear. Additional debridement was performed 2 weeks later revealing exposure of the left condyle without bony destruction along with left tympanomandibular joint fibropurulent material penetrating through the middle ear. The exposed wound was initially covered with temporary expander flap and was later reconstructed with skin graft and temporoparietal fascia flap.
Myiasis refers to parasitic infestation of body cavity by fly larvae. Although rare, myiasis is highly relevant to otolaryngologists as the disease commonly affects head and neck regions including ears, oral cavity, nose, sinuses, and lymph nodes. 1,2 This case reports a rare advanced presentation of aural myiasis with extensive soft tissue and cartilage destruction exemplifying the potential destructive nature of myiasis. Presentations of aural myiasis in previous reports have been mostly during early stages involving isolated areas of the middle ear, tympanic membrane, external auditory canal, or partial pinna. 2 –4 The patient in this report had a history of schizophrenia which likely has delayed the diagnosis and treatment of the infestation during early stage.
Early stages of aural myiasis can be treated with maintaining simple aural toilet with suction and topical and/or oral antibiotic coverage. 5 Localized tissue hypoxia can be created with application of viscous liquid (eg, normal saline, 70% ethanol, 10% chloroform, oil drops, urea, dextrose, creatine, topical ivermectin, and iodine saline) and larvae can be suctioned and expelled from submucous membrane by applying pressure. In Bolivia, general anesthesia is often used for larvae extraction for patient comfort.
Late stage aural myiasis, as in this case, warrants extensive surgical debridement of the infected tissue and reconstruction. Although there has not been a protocol established for advanced myiasis treatment, ivermectin can be used for complicated cases prior and/or after extraction (eg, single dose of mectizan 6 mg or ivermectin 200 µg/kg prior to extraction, dose up to 300 µg/kg for 3 consecutive days). Pain often resolves within 24 hours of treatment initiation. Systemic antibiotic treatment is indicated in advanced cases with purulent otorrhea or when involving deep cavities. Surgical management with mastoid exploration is advised when maggots are deeply embedded and difficult to expel (eg, when maggots are identified in the middle ear space through the perforated tympanic membrane or when cerebral myiasis is suspected). 2,6
Otologic complaints secondary to myiasis can have serious downstream sequelae such as hearing loss, meningitis, seizure, and death warranting high suspicion for diagnosis and treatment in patients who may have myiasis based on the history and examination.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.