
Abstract

A 78-year-old otherwise healthy Caucasian male presented to our ENT clinic with a 4-week history of intermittent odyno–dysphagia and globus pharyngeus. The patient denied tobacco and alcohol consumption. He presented a noticeable hot potato voice. His physical examination revealed a left palpable 1.5 cm level IIa lymphadenopathy, and his flexible laryngoscopy showed a brown polypoid pedunculated mass in the left pyriform sinus. The patient also mentioned a bump on his right posterior thigh that had been present for 2 years without any change in size, causing him major discomfort when sitting. It was a 6 × 4 cm, nonsuspicious-looking, subcutaneous, dome-shaped purple lesion.
A contrast-enhanced computed tomography (CT) of the neck showed a well-circumscribed 1.5 × 0.8 cm left pyriform sinus mass in addition to an ipsilateral 1.6 cm level IIa necrotic lymphadenopathy (Figure 1). A rigid laryngoscopy was performed under general anesthesia and allowed excisional biopsy of a 2.3 × 1.6 × 0.8 cm brown-colored, pedunculated lesion of the medial wall of the left pyriform sinus (Figure 2). A concomitant complete excision of the right posterior thigh lesion was also performed (Figure 3). Both surgical specimens were sent for routine pathology.
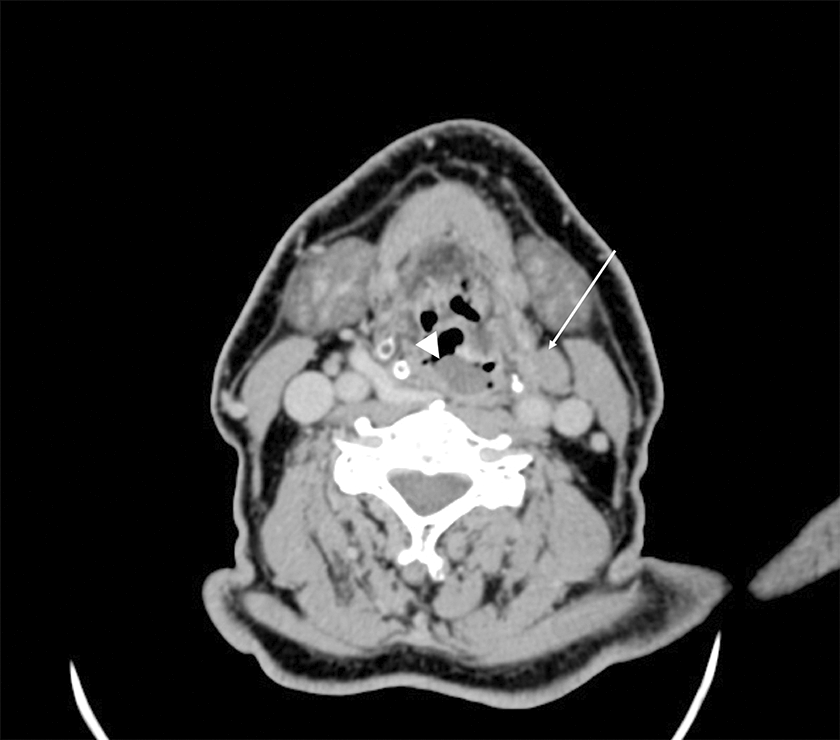
Axial contrast-enhanced cervical CT scan showing a 1.5 × 0.8 cm well circumscribed lesion of the left pyriform sinus (arrowhead), in addition to an ipsilateral 1.6 cm level IIa necrotic lymphadenopathy (arrow). CT indicates computed tomography.

A, Peroperative direct laryngoscopy image showing a 2.3 × 1.6 × 0.8 cm brownish pedunculated lesion of the left pyriform sinus. B, Surgical specimen sent to routine pathology.

Right posterior thigh dome-shaped red mass.
Histological examination of the thigh mass showed a blue round cell tumor arranged in sheets. The cells exhibited scant cytoplasm and round vesicular nuclei with granular chromatin. Mitotic figures were numerous. Immunohistochemistry stains showed a dot-like positivity with pan-cytokeratin (AE1/AE3) and CK20. The tumor cells were positive for neuroendocrine markers (synaptophysin and chromogranin A) in a diffuse, granular cytoplasmic pattern. Histological examination of the pyriform sinus mass revealed a largely necrotic round cell tumor that stained positive for pan-cytokeratin (AE1/AE3), CK20, and neuroendocrine markers. Both lesions were consistent with Merkel cell carcinoma (MCC), and the hypopharyngeal location was considered a metastasis of the primary cutaneous carcinoma.
The patient underwent a full metastatic workup consisting of a brain magnetic resonance imaging and a positron emission tomography CT scan, which did not reveal any additional suspicious lesion. He was diagnosed with metastatic MCC and was referred to the oncology department where he was offered a VP16-Cisplatin-based chemotherapy regimen. The patient was then lost to follow-up.
Merkel cell carcinoma is an uncommon, highly aggressive, primary cutaneous neuroendocrine tumor originating from the epidermal neurocutaneous mechanoreceptors called Merkel cells. Toker was the first to describe this skin neoplasm in 1972. 1 It commonly affects sun-exposed areas in the elderly and immunosuppressed individuals, and it presents as a red violet cutaneous tumor nodule that is typically dome-shaped or plaque-like. 2 During the last 2 decades, the worldwide incidence of MCC has been increasing steadily due to the increasing age of the population and the rise in sun exposure. In addition, cutaneous lesions are readily biopsied or excised, and the widespread use of immunohistochemistry has facilitated its diagnosis. Merkel cell carcinoma is a locally aggressive tumor and commonly presents at an advanced stage due to delay in diagnosis. At the time of presentation, regional lymph node involvement can be seen in 27% of patients, and distant metastasis in 7% of cases. 3
Merkel cell carcinoma is frequently found on extremities and in the head and neck region. The differential diagnosis of MCC consists primarily of other round blue cell tumors including melanoma, lymphoma, leukemia, small cell carcinoma, alveolar rhabdomyosarcoma, and primitive neuroectodermal tumors. Immunohistochemistry plays a major role in the diagnosis of MCC; the tumor stains positive for CK20, chromogranin A, synaptophysin, and neuron-specific enolase but negative for thyroid transcription factor 1, CD45, CD3, myeloperoxidase, desmin, and S100. 4
The mainstay of treatment is a wide surgical resection, with most authors agreeing on a 1 to 2 cm margin. Adjuvant radiation therapy to the primary tumor site is commonly indicated and allows better local control. Chemotherapy is used mostly in metastatic and palliative cases.
Merkel cell carcinoma of the head and neck skin has been frequently reported to metastasize to the parotid gland. 5 However, head and neck metastasis of an extremity MCC is extremely rare. Only 2 cases of oropharyngeal metastasis and 1 case of oral metastasis have been reported, so far, and all 3 of them were late metastatic recurrences from an already known and surgically treated MCC. 6 -8 Moreover, metastatic disease to the pyriform sinus is exceptional; our literature review revealed only a few case reports including metastatic breast carcinoma, colon carcinoma, hepatocellular carcinoma, and primary malignant mesothelioma. To our knowledge, this is the first reported case of a pyriform sinus metastasis from MCC.
Footnotes
Authors’ Note
All authors have equal contribution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.