
Abstract

A 65-year-old African American male retired shipyard worker with chronic obstructive pulmonary disease and a long history of tobacco abuse presented for evaluation of questionable lymphadenopathy. He denied any other complaints including dysphonia, dysphagia, neck pain, or weight loss. His otolaryngologic history and family history were unremarkable. Flexible fiber-optic laryngoscopy revealed laryngeal hyperpigmentation of the interarytenoid region, aryepiglottic folds, and postcricoid region (Figure 1). Direct laryngoscopy with biopsy was performed to rule out malignancy given his prolonged history of tobacco abuse. Histopathology identified benign pigmented squamous epithelium consistent with laryngeal melanosis (LM). No further treatment other than smoking cessation was recommended. On 1-month follow-up, he remained asymptomatic and demonstrated stable findings on laryngoscopy. He elected to undergo close observation with surveillance visits every 3 months.
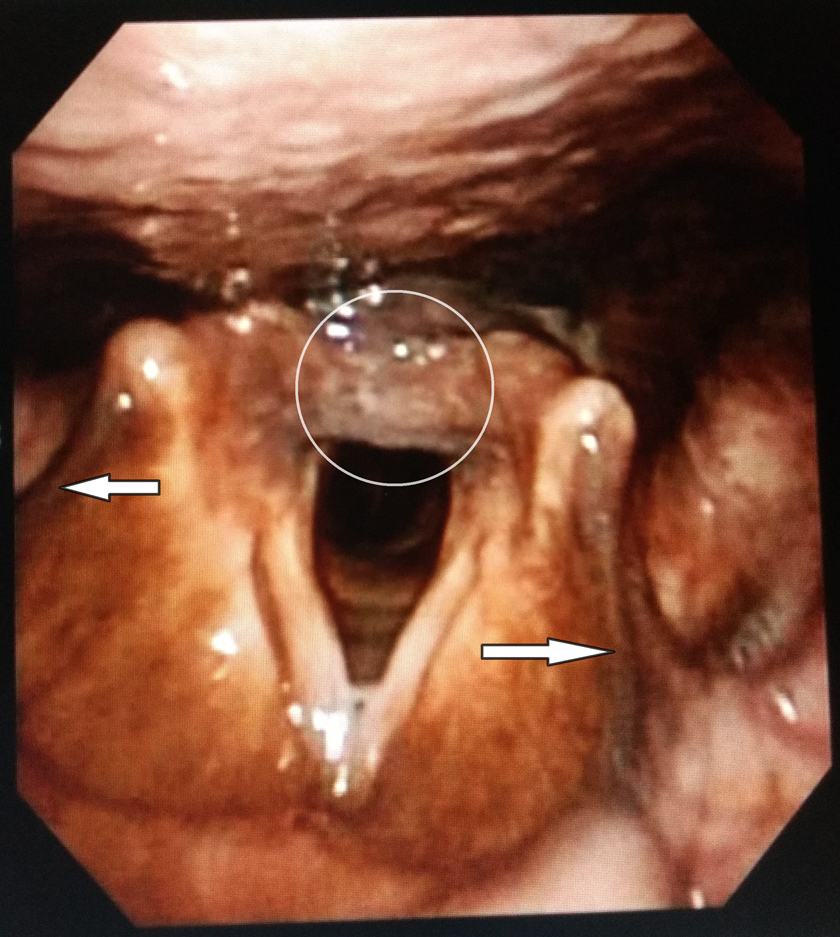
Flexible fiber-optic laryngoscopy shows mucosal hyperpigmentation of the interarytenoid and postcricoid region (circle), as well as the aryepiglottic folds (arrows).
Laryngeal melanosis is defined by the presence of ectopic melanocytes within the laryngeal epithelial lining and characterized by laryngeal mucosal hyperpigmentation. 1,2 Despite its initial depiction by Goldman in 1972, 3 LM remains a poorly described entity of the head and neck with less than 40 cases reported in the literature. 2 The pathophysiology remains unclear, but tobacco smoke may be responsible for the accumulation of nicotine in melanin-containing tissues, and this retention may increase melanin synthesis. 4 Laryngeal melanosis tends to affect African Americans, males, and smokers in the seventh decade of life. Dysphonia is the most common presenting symptom, although the LM usually is not causally related to the dysphonia. Laryngoscopy reveals brown laryngeal mucosa discoloration which can affect any subsite of the larynx. 2,5 The reported association between LM and upper aerodigestive tract malignancy (42% 5 to 50% 2 ) warrants a close examination for head and neck malignancy. Microlaryngoscopy with biopsy is not always mandatory, but should be reserved for cases with persistent symptoms or suspicious laryngeal findings. 2 Increased physician awareness of this rare but distinctive lesion may not only aid early cancer diagnoses but also avoid unnecessary surgical interventions.
Footnotes
Authors’ Note
The manuscript herein reports a patient’s encounter at Tulane University Medical Center. This manuscript was submitted as a poster presentation for the upcoming 2018 AAOHNS Annual Meeting in Atlanta, Georgia, on October 7-11.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.