
Abstract

The author presents the case of a 59-year-old man who presented to the clinic with a 5-month history of a rapidly growing and painful mass of the anterior mandible that was initially presumed to be due to dental infection. He had a 40-pack-year smoking history. He also reported unintentional weight loss of 10 pounds over the last 3 months. The patient’s past medical history was remarkable for type 2 diabetes, hypertension, and asthma. Contrast-enhanced computed tomography (CT) demonstrated a diffusely infiltrating mass involving the anterior mandibular gingiva with gross invasion of the mandible and extending posteriorly into the root of the tongue (Figures 1 and 2). Biopsy proved well-differentiated squamous cell carcinoma (SCC). 18F-fluorodeoxy glucose positron emission tomography with CT (FDG-PET/CT) demonstrated a highly FDG-avid lesion corresponding to the invasive mandibular lesion. There was also increased FDG uptake that corresponded to the right- and left-sided level IB lymph nodes seen on the enhanced CT (Figure 3).
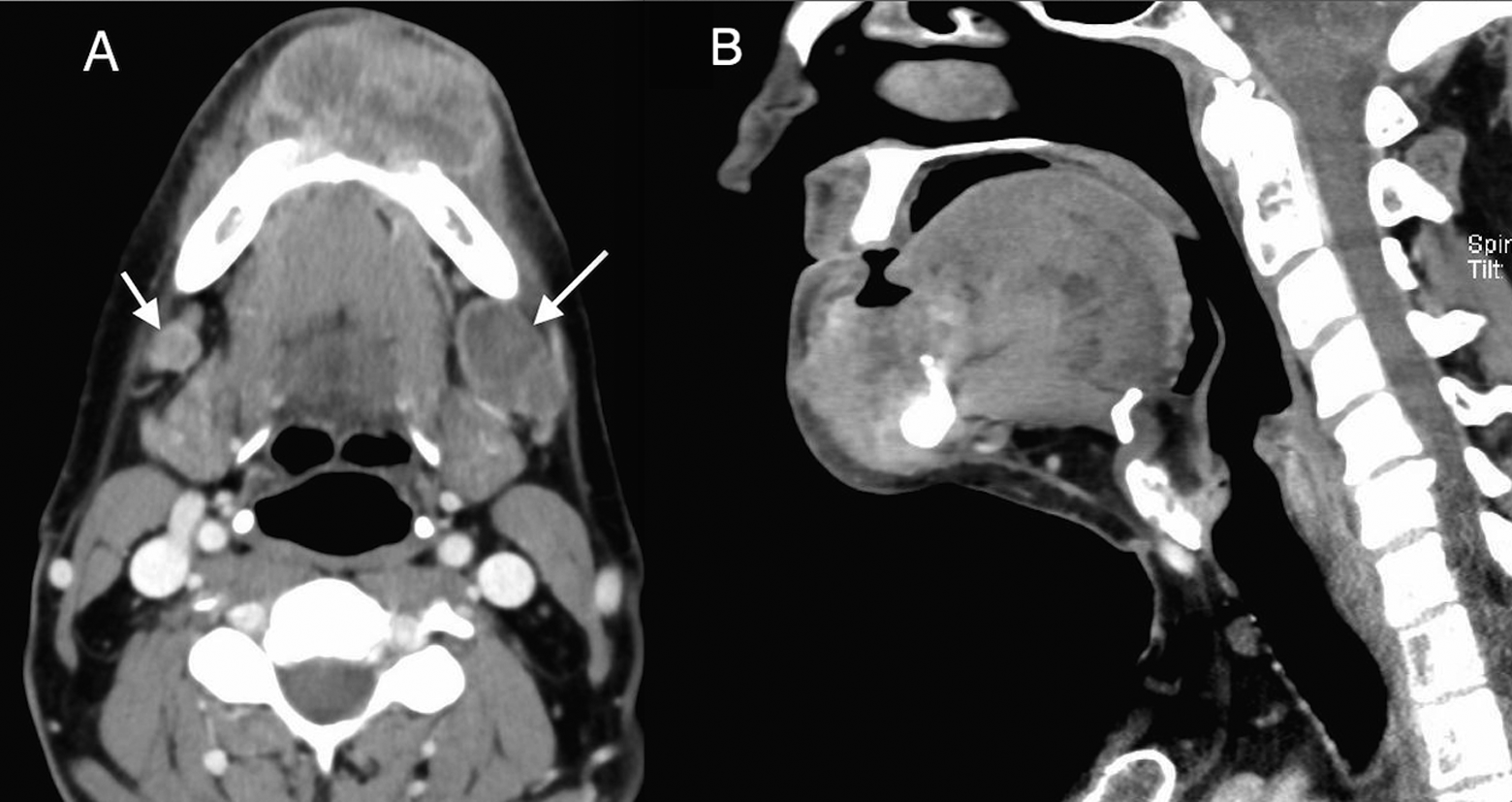
Axial (A) and sagittal (B) soft-tissue window images from a contrast-enhanced computed tomography (CT) scan demonstrate a large heterogenous soft-tissue attenuation lesion in the anterior mandible invading the floor of the mouth and the root of the tongue. Necrotic areas appear hypodense with peripheral enhancement. Posteriorly, the lesion has ill-defined infiltrative margins. Note the necrotic left level IB node that measures 3 cm (long arrow). Another subcentimeter lymph node in the right level IB, concerning for metastasis (short arrow).

Axial bone window image from a contrast-enhanced computed tomography (CT) scan demonstrate gross invasion of the mandible and complete cortical breakthrough on both sides (T4a).
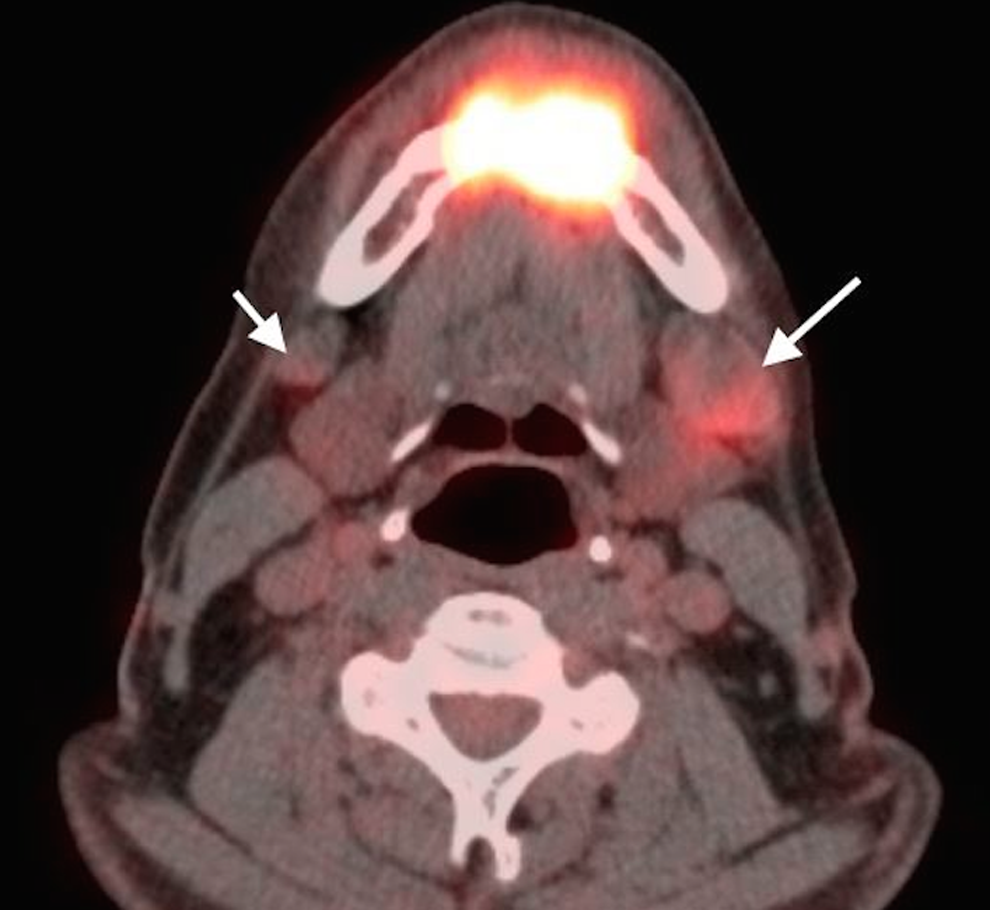
Fluorodeoxy glucose positron emission tomography computed tomography (FDG-PET/CT) axial image reveals a highly FDG-avid lesion corresponding to the invasive lesion in the anterior mandible. There is a prominent left-sided level IB lymph node, demonstrating mild FDG uptake, consistent with nodal metastasis (long arrow). Another smaller lymph node in the right level IB region is mildly hypermetabolic, likely metastatic in nature (N2c) (short arrow). These findings were confirmed by biopsy. There is no evidence of distant metastasis (M0).
The patient has undergone a composite resection of the tumor with neck dissection and free flap reconstruction followed by chemoradiation therapy. Squamous cell carcinoma accounts for more than 90% of oral cavity and oropharyngeal malignancies. 1 Accurate identification and reporting of key imaging findings allow the radiologist to accurately determine the extent of disease and help clinicians plan appropriate treatment.
Computed tomography is the modality of choice for initial imaging of oral SCC and should be performed with iodinated intravenous contrast to increase tumor enhancement and conspicuity unless contraindicated for medical reasons (eg, renal disease or contrast allergy) or therapeutic reasons (eg, planned use of radioactive iodine for thyroid cancer).
Computed tomography is excellent for evaluation of cortical bone involvement and detection of nodal metastasis and extracapsular tumor spread. Accurate delineation of tumor boundaries can be difficult in areas where enhancing tumor has similar attenuation characteristics to adjacent soft tissues. 2
Computed tomography images are often degraded by streak artifact from dental amalgam, although better visualization of regions can be improved by image acquisition in a different angle plane.
Superficial lesions in the oral vestibule are best assessed by having the patient puff the cheeks outward during image acquisition. This maneuver results in separation of the mucosal surfaces in the vestibule, allowing for better visualization.
Magnetic resonance (MR) imaging is superior to CT in delineation of the tumor margins and identification of perineural spread of disease. Gadolinium is used as a contrast agent to enhance the definition of soft tissues.
Fluorodeoxy glucose-PET imaging is particularly helpful in identification of distant metastases and detection of synchronous and unknown primary tumors. The FDG-PET/CT is superior to CT or MR imaging alone for initial detection of nodal metastasis and for evaluation of recurrent disease. One limitation of PET-CT is the inability to differentiate between tumor and inflammation, as both conditions are associated with hypermetabolic activity reflected by increased FDG uptake. 3
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.