
Abstract

A 27-year-old man presented with a 5 day history of dysphonia after an episode of vigorous singing. He was a tenor opera student having difficulty with his lower register. He also had a chronic complaint of frequent throat clearing. Additionally, he noted a history of occasional heartburn symptoms for which he took a proton pump inhibitor (PPI) intermittently. On examination, the patient had difficulty sliding down from falsetto to modal voice. He had a Singing Voice Handicap Index of 7. He had Reflux Symptom Index of 5.
Strobovideolaryngoscopy showed evidence of reflux including laryngeal erythema, moderate edema, posterior commissure hypertrophy, and endolaryngeal mucus. The Reflux Finding Score was 12. Three points of localized erythema and edema were also identified on the mucosa overlying the anterior tips of the arytenoid cartilages bilaterally and on the laryngeal surface of the epiglottis at the petiolus (Figure 1). These areas represent 3 contact points from chronic throat clearing and severely hyperfunctional muscle tension dysphonia.
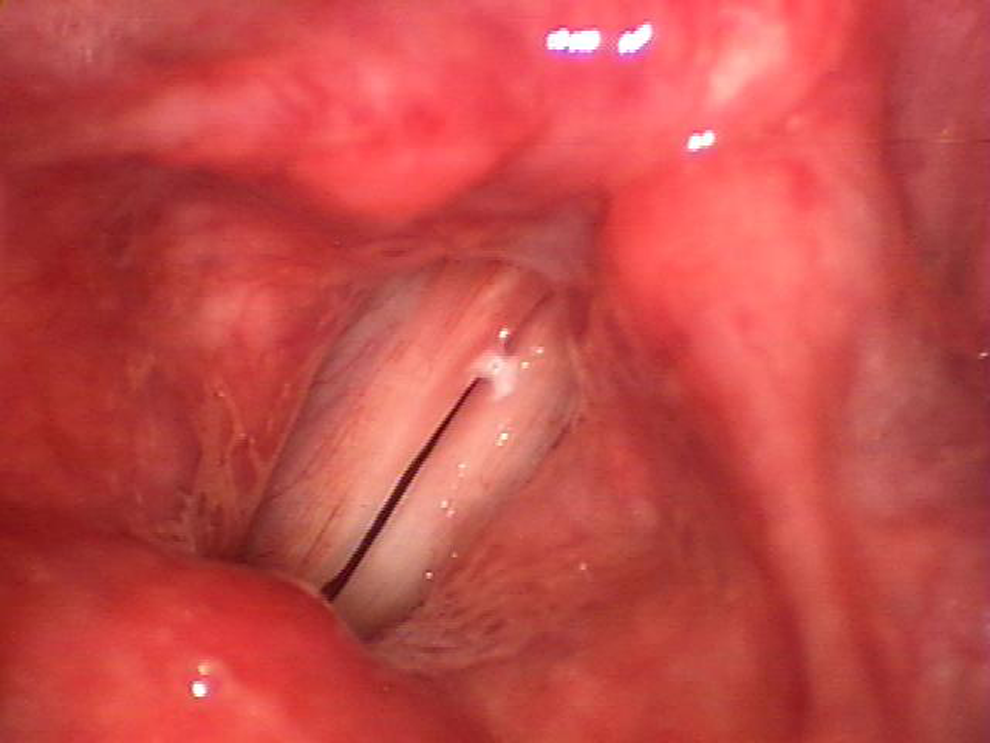
The videostroboscopic image illustrates erythematous regions of mucosa along the anterior surfaces of both arytenoid cartilages and the laryngeal surface of the epiglottis in the area of the petiolus.
Additional findings included moderate stiffness of the right true vocal fold with an area of white, avascular tissue along the vibratory margin. The left true fold showed mild stiffness and decreased vibratory function along with a sulcus at the vibratory edge. These glottis findings likely resulted from phonotrauma.
The most common symptoms of laryngopharyngeal reflux include voice complains, throat clearing, chronic cough, and postnasal drip. 1 Studies suggest that acid reflux is present in 25% to 50% of patients with globus sensation. 2 Although this has been well studied, throat clearing is often still misdiagnosed. Additionally, it is important to note that throat clearing can become self-perpetuating. Chronic irritation to the anterior surfaces of the arytenoids and laryngeal surface of the epiglottis can cause the sensation of a need for further throat clearing. As such, it is imperative to recognize not only laryngopharyngeal reflux findings on strobovideolaryngoscopy but also signs of additional frequent throat trauma and to treat accordingly.
Our patient was treated with twice daily PPI, ranitidine, prednisone 60 mg daily, and voice rest for 1 week. With this multimodal approach, we were able to calm the cycle of irritation and inflammation causing dysfunction. Voice rest was followed immediately by voice therapy which we also believe to be imperative in treatment and prevention of further trauma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.