
Abstract

Neurofibromas are benign nerve sheath lesions of the peripheral nervous system. They account for 0.03% to 0.1% of benign tumors of the larynx. 1 Fewer than 40 cases have been documented in the English literature, the vast majority being neurofibromatosis type 1 (NF1) in the supraglottis of pediatric patients. 2 Gstöttner et al (2005) described the first case of isolated neurofibroma of the larynx in the subglottic region, resected by CO2 laser. 3 The only previous neurofibroma of the vocal fold occurred in a 78-year-old male who presented with a 1-month history of hoarseness and odynophagia, resected by cold steel. 2 We present the second documented case of isolated laryngeal neurofibroma of the vocal fold, which became symptomatic over years rather than months.
A 48-year-old lady was referred to the otolaryngology clinic with a 5-year history of progressive dysphonia, but no dysphagia or odynophagia. She was a long-term smoker but did not drink alcohol. She had a history of reflux disease and obesity and no significant family history. Flexible nasopharyngolaryngoscopy revealed Reinke’s edema and a subcentimeter right vocal fold lesion. The remainder of the head and neck examination was normal. She underwent microlaryngoscopy (Figure 1A and B), cold steel excision of the lesion, and reduction of Reinke’s edema. Jet ventilation was converted to endotracheal intubation due to difficulty ventilating as a result of the patient’s body habitus.
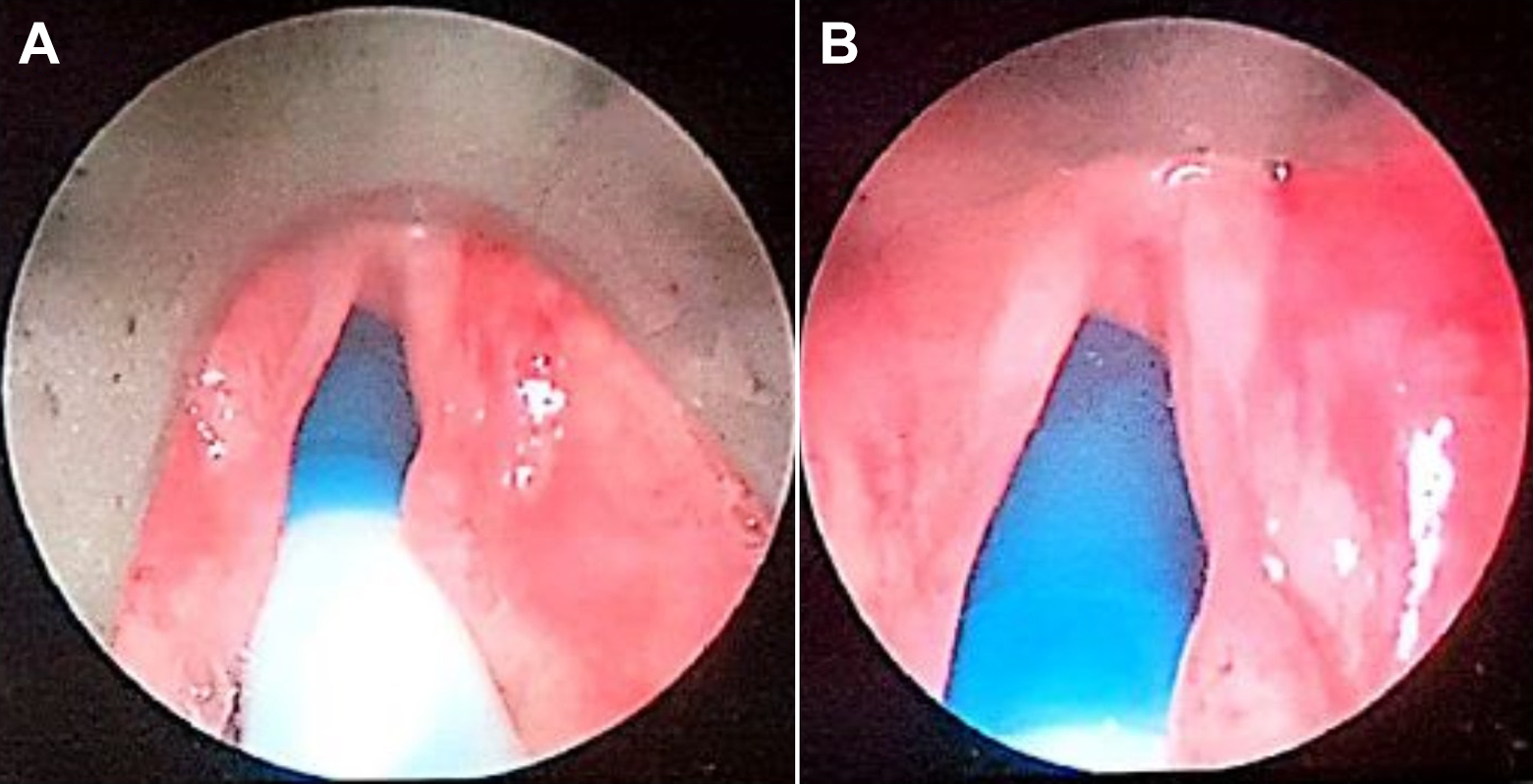
A, Vocal fold neurofibroma with associated Reinke’s edema. B, Vocal fold neurofibroma with associated Reinke’s edema (magnification ×2).
At 3-month follow-up, her dysphonia had improved substantially and laryngeal appearance was normal. Histology of the polyp confirmed laryngeal neurofibroma (Figure 2). Diagnostic features included slender spindle cells embedded within a variable collagenous stroma, alongside small nerve fibers and axons. Immunohistochemical staining demonstrated strong positivity to S100 (due to neurogenic origin) and CD34. The patient was referred to the neurofibromatosis clinic, where systemic neurofibromatosis was ruled out, and a diagnosis of isolated laryngeal neurofibroma was confirmed.
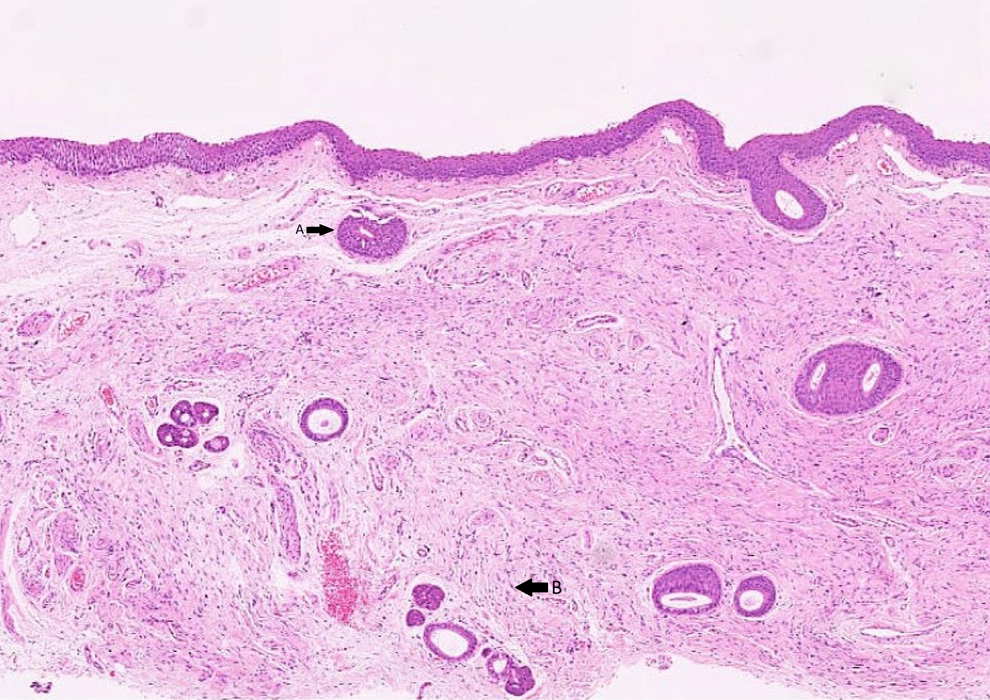
Hematoxylin and eosin stain of the laryngeal neurofibroma, ×25. Peripheral nerves (Arrow A) and spindle cells (arrow B) with “shredded carrot” appearance.
Isolated neurofibroma of the larynx is extremely rarely. The only previous vocal fold neurofibroma in the literature presented with subacute dysphonia. 2 Our patient presented with a progressive onset of symptoms over 5 years, suggesting a slow-growing lesion. Almost all patients with NF1 are diagnosed by 8 years old, 4 which contrasts with the middle-age presentation of isolated laryngeal neurofibromas. Neurofibromas can occur in the larynx without features of neurofibromatosis, but thorough examination of all systems is necessary. Therefore, a multidisciplinary approach is essential for diagnosis and management, ideally with involvement of a tertiary neurofibromatosis service. Laser or cold steel resection is an acceptable definitive treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.