
Abstract
A 47-year-old Chinese man who had repeated left nasal congestion, the hyposmia and occasional bleeding in the snivel more than 10 years, presented to our hospital for the persistent left nasal congestion during the past 6 months. The patient denied the history of definite diagnosis or special treatment.
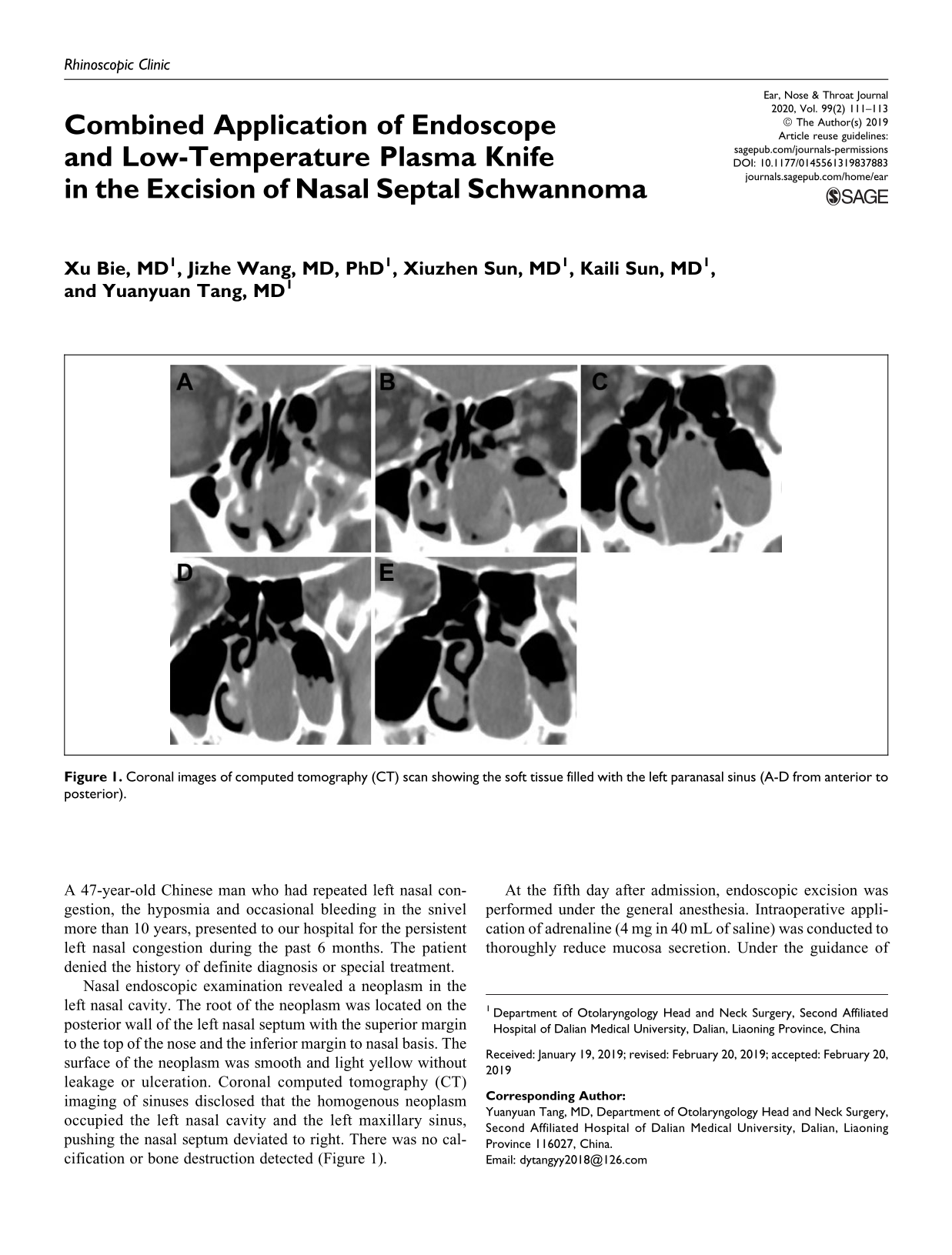
Nasal endoscopic examination revealed a neoplasm in the left nasal cavity. The root of the neoplasm was located on the posterior wall of the left nasal septum with the superior margin to the top of the nose and the inferior margin to nasal basis. The surface of the neoplasm was smooth and light yellow without leakage or ulceration. Coronal computed tomography (CT) imaging of sinuses disclosed that the homogenous neoplasm occupied the left nasal cavity and the left maxillary sinus, pushing the nasal septum deviated to right. There was no calcification or bone destruction detected (Figure 1).
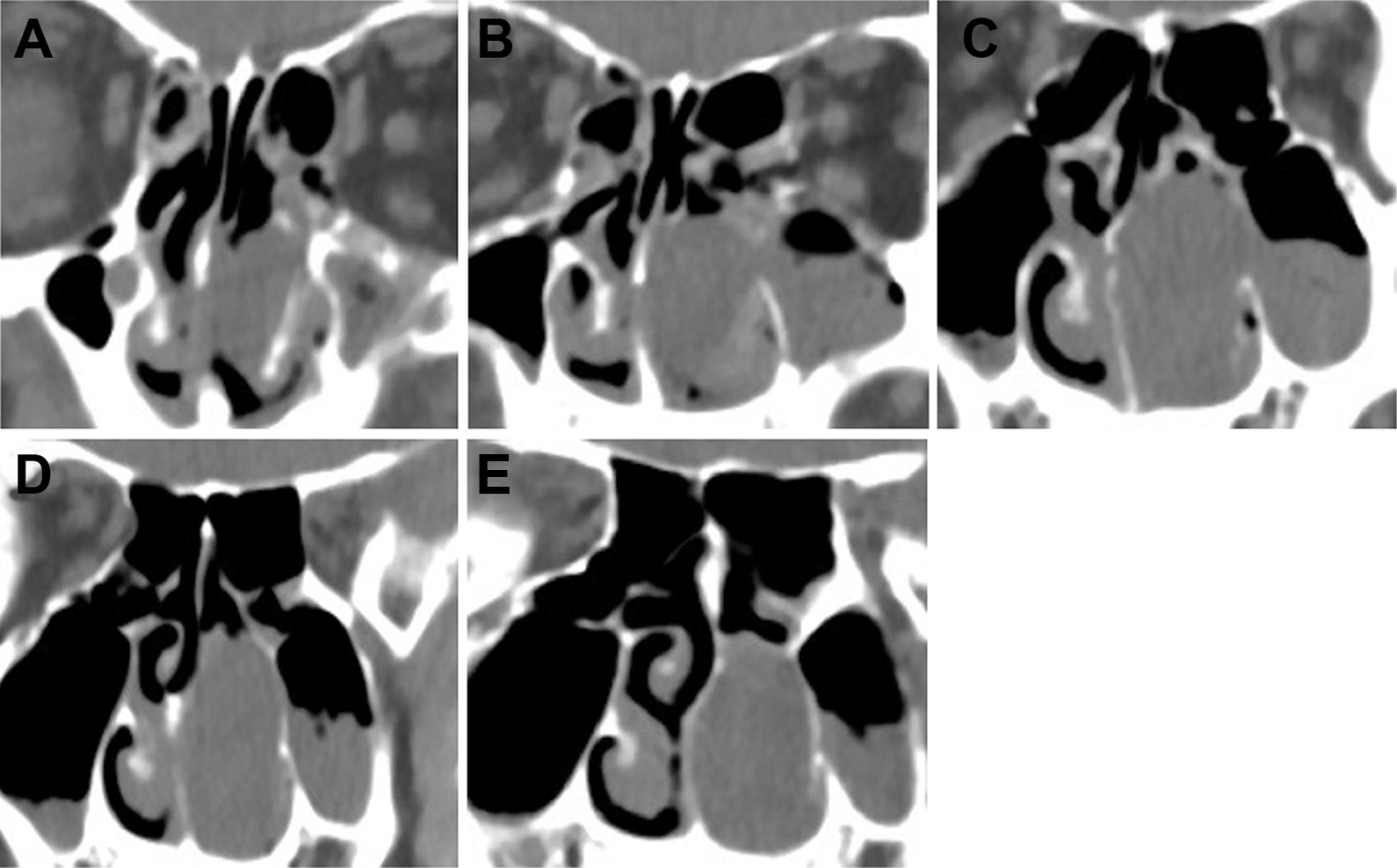
Coronal images of computed tomography (CT) scan showing the soft tissue filled with the left paranasal sinus (A-D from anterior to posterior).
At the fifth day after admission, endoscopic excision was performed under the general anesthesia. Intraoperative application of adrenaline (4 mg in 40 mL of saline) was conducted to thoroughly reduce mucosa secretion. Under the guidance of endoscope, a low-temperature plasma knife (MECHAN, MC401, MECHAN Co.Ltd. Chengdu, CHINA) was used to cut the mucosa at 0.5 cm away from the neoplasm root. Then, mucosa along the neoplasm root was striped and cut to remove neoplasm without damaging the septal cartilage and bone (Figures 2 and 3A). The wound was covered with Nasopore containing erythromycin ointment.
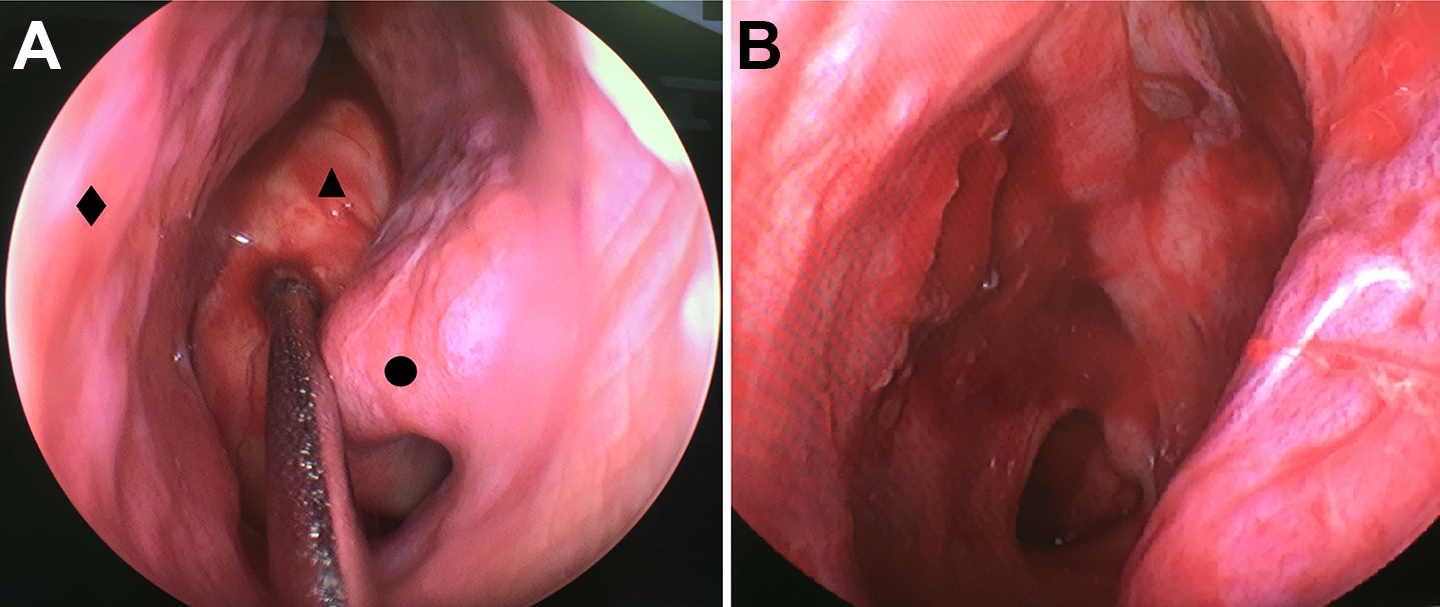
Nasal endoscopic observation in preoperation (A) and postoperation (B). (Triangle in A represents the neoplasm, round dot stands for concha nasalis inferior, rectangle indicates nasal septum).
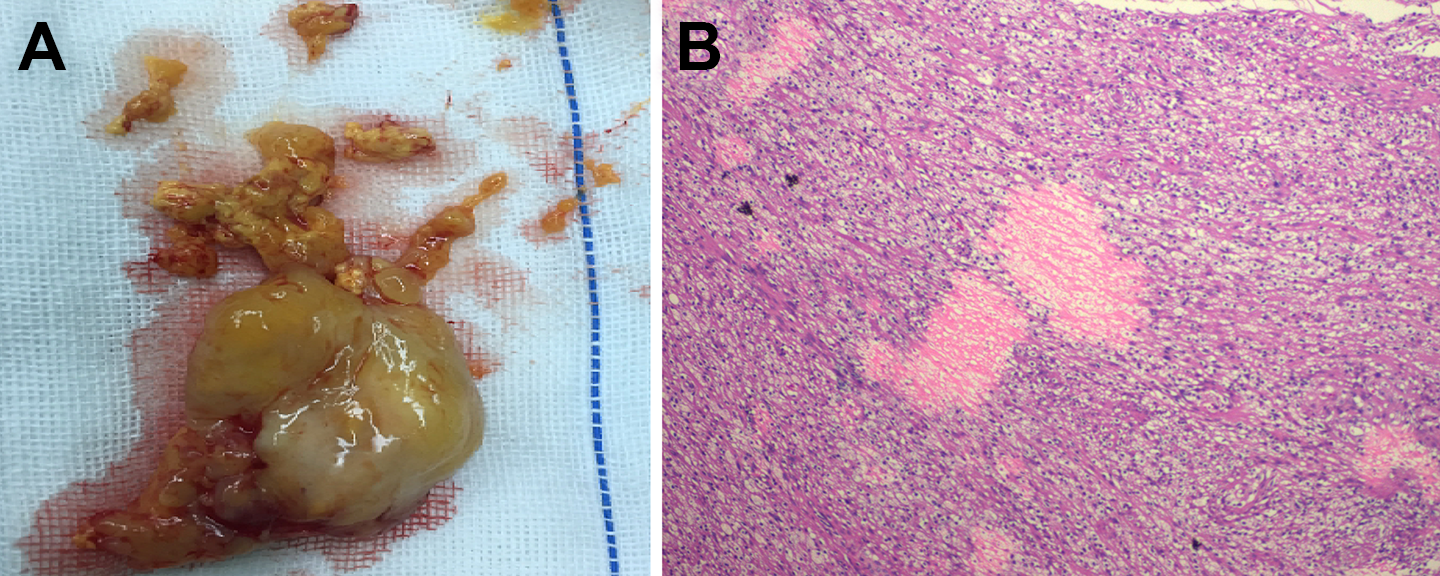
The gross specimen of the neoplasm after excision (A) and paraffin section of the neoplasm (B). H&E staining (40×).
Histopathological examination showed that a typical feature of schwannoma. The focal fusiform cells were arranged in bundles and rich in transparent cytoplasm with the small round nucleus (Figure 3B).
After 2 months of the surgery, endoscopic observation confirmed that the wound mucosa in nasal septum was smooth and completely covered by epithelium. Within 6 months after the surgery, the olfaction of patient recovered and no nasal congestion or bleeding took place. The patient remained free of neoplasm in the nasal cavity and sinus.
Schwannoma is a benign neurogenic neoplasm originating from the schwann cells and insensitive to radiotherapy and chemotherapy. 1,2 There are only 18 cases of nasal septal schwannoma reported in the English-written literatures from 2000. 3,4 Therefore, surgical resection is the optimal choice with the higher success and lower recurrence ratios. Taking the advantages of the developing minimally invasive procedures, nasal endoscopy have being applied more and more widely in nasal and sinus surgery. 5
In tissue excision, low-temperature plasma knife is able to reduce tissue damage and postoperative pain and edema effectively, by decreasing damage in deep tissue or heat injury of parenchyma. Bleeding is also reduced by local hemostasis resulting from scar contraction and the low-temperature thermal effect. 6 In head and neck surgery, the utmost concern is the injury of cranial nerves. Low-temperature plasma knife can cause less nerve injury because of the less thermal effect, which makes it the optimal choice in the dissecting nerve surrounding tissues. Therefore, combined application of nasal endoscopy with the low-temperature plasma knife in nasal surgery will decrease the operative damage and enhance of postoperative mucosal recovery and epithelialization.
The main manifestations of nasal schwannoma are progressively unilateral nasal congestion and bulging, ipsilateral hyposmia, local pain, and intermittent epistaxis, which were determined by the location and size of the neoplasm. Schwannoma can also be determined by the surrounding bones by its large size, which confuses the benign schwannomas with other malignant neoplasms. Therefore, the endoscopic observation and CT images are insufficient for the diagnosis of schwannoma, and the pathological examination is indispensable to distinguish benign schwannomas from the malignant nasal tumors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China (Grant No. 31500764, 11472074 and 11772087).