
Abstract

Case
A 27-year-old male patient presented to our department with intermittent alteration of voice quality that had deteriorated gradually over the preceding 3 years. He experienced “hot potato” voice rather than any dyspnea or hoarseness. Clinical examination of the head and neck did not reveal any pathology; however, flexible laryngoscopy showed a large, smooth, orange-yellow mass occupying the lower supraglottic area, mainly located on the left aryepiglottic fold, false vocal fold, and right arytenoid area. The size of the lesion caused sealing of the laryngeal inlet on phonation (Figure 1). The patient underwent microlaryngoscopy and excisional biopsy, the specimens were stained with Congo red, and the pathological examination was consistent with amyloidosis (Figure 2A and B). Subsequently, the patient was tested thoroughly in order to rule out systemic disease (chest X-ray, computed tomography scan of the neck, electrocardiogram, cardiac ultrasound, urine test, blood tests, specific tests for identifying monoclonal proteins in the serum and urine). Detection of a small quantity of κ chains in the blood and urine samples led us to proceed with bone marrow biopsy which was negative for systemic amyloidosis. Finally, the pathology was characterized as isolated laryngeal amyloidosis. He underwent a microlaryngoscopy and cold instrument resection-staged procedure of the lesion (the first procedure involved excisional biopsy and the second excision of the residual lesion). We put the patient under 6 monthly follow-up which included clinical examination and transnasal laryngoscopy. As the lesion almost spared the true vocal fold, the postoperative voice quality was very satisfactory (Figure 3). After 2 years, the patient remains recurrence free. Informed consent has been obtained by the patient prior to publication.
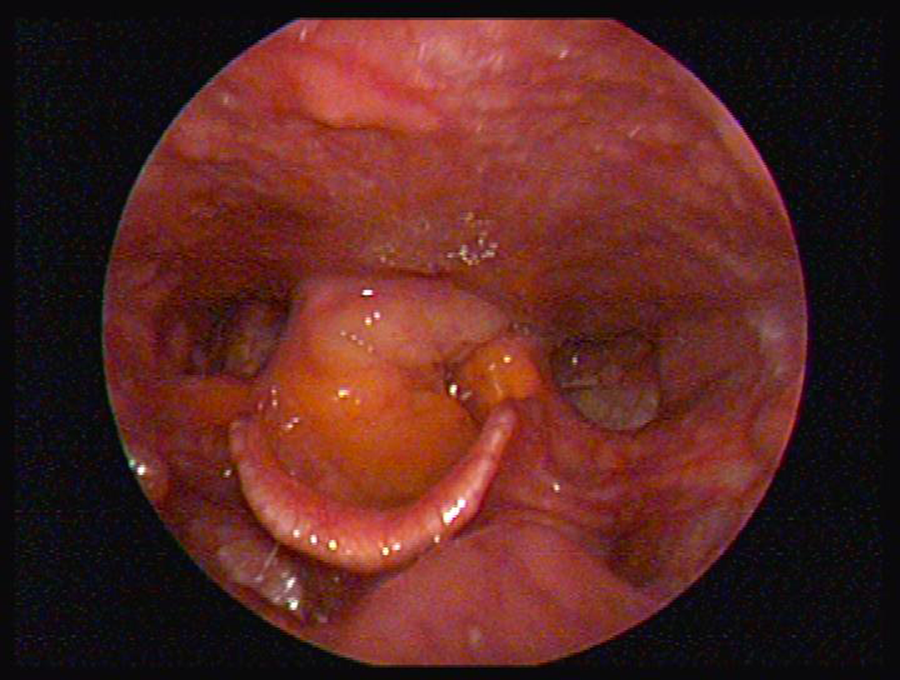
Preoperative endoscopic image depicting a yellowish supraglottic lesion, occupying the right aryepiglottic fold, false vocal fold, and left arytenoid. On vocal fold adduction, sealing of the laryngeal inlet at a supraglottic level was responsible for patient’s voice symptoms.
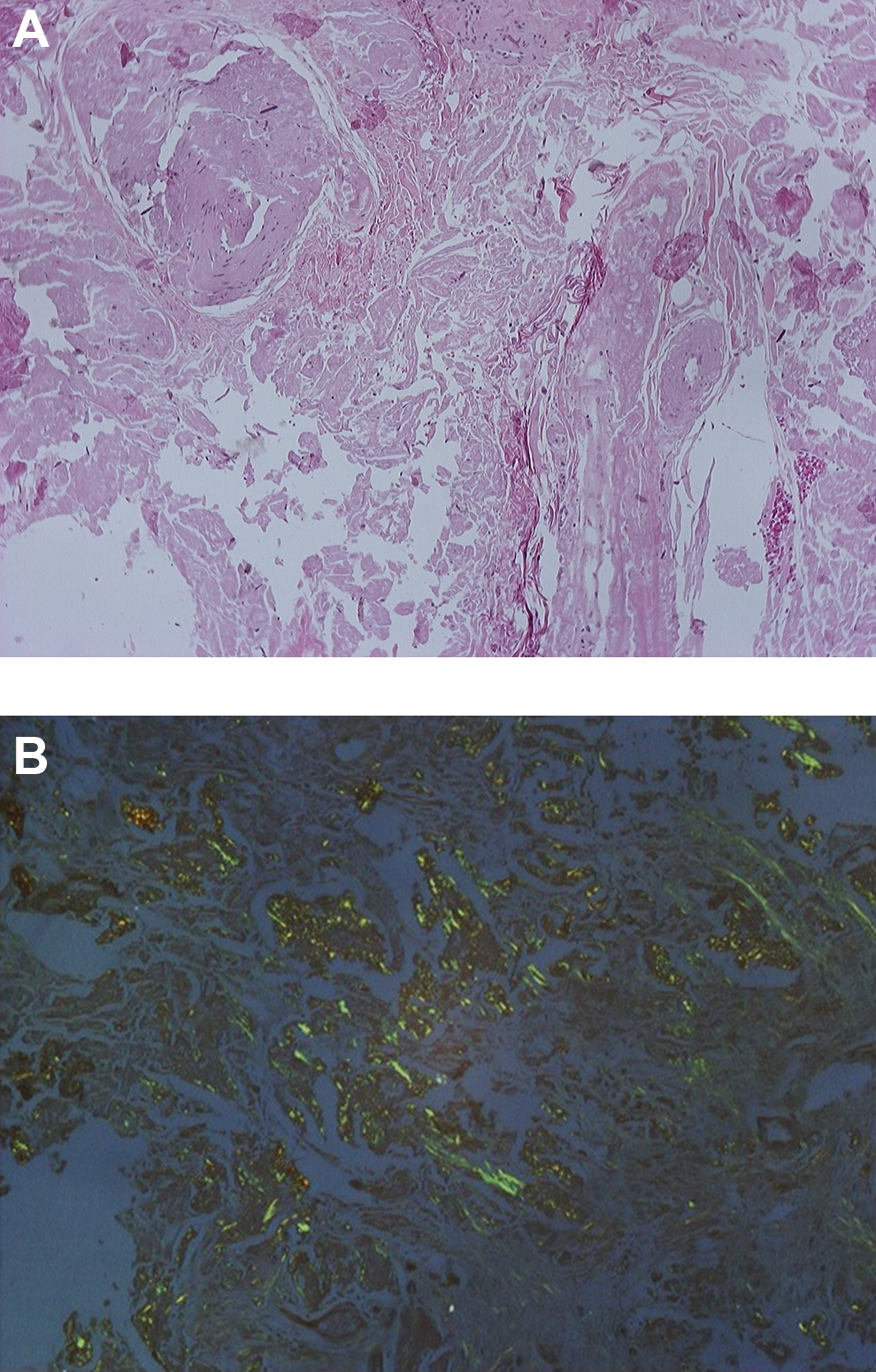
Histological picture of the laryngeal lesion after (A) HE staining and (B) Congo red staining.
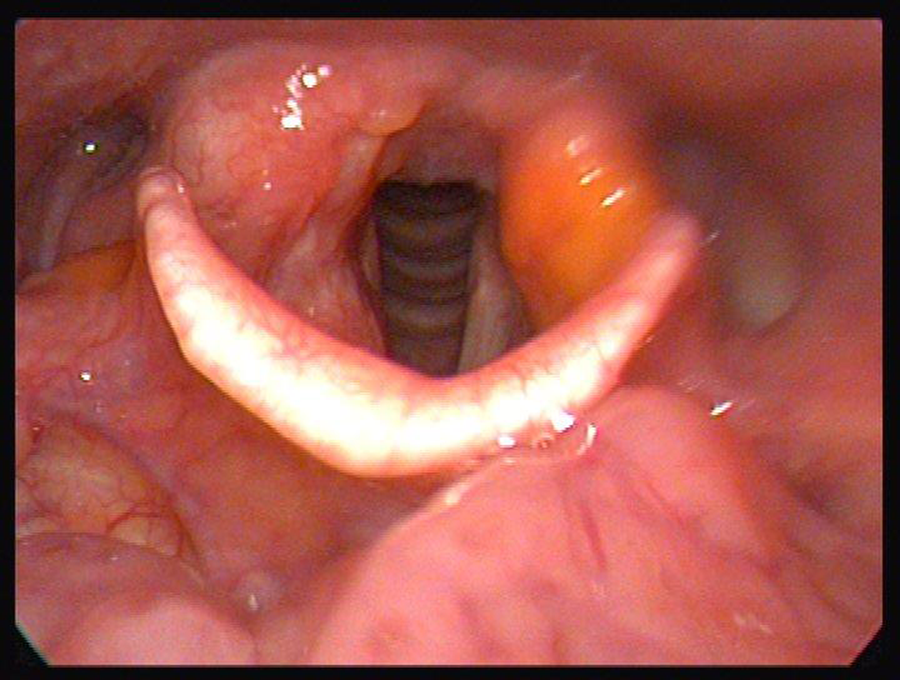
Postoperative image of the laryngeal inlet showing a patent glottis.
Discussion
Differential diagnosis requires attention as laryngeal amyloidosis has no specific clinical characteristics. It is essential to exclude malignant masses, such as squamous cell carcinoma and medullary carcinoma of the thyroid that has invaded the larynx, as well as other non-neoplastic lesions. Sarcoidosis, lymphoma, chondrosarcoma, polyps may mimic laryngeal amyloidosis. 1 Other conditions that involve amyloid deposition and need to be differentiated are secondary amyloidosis, extramedullary plasmocytoma, multiple myeloma, and neuroendocrine carcinoma. 1
Amyloidosis is a slow growing, benign process that is characterized by extracellular fibular protein deposition. Clinically, amyloidosis can be systemic or localized to a single organ. 2 As far as the upper aerodigestive tract is concerned, 2 forms of amyloid deposition have been described: tumor nodules and diffuse subepithelial deposition, with the first being the commonest in laryngeal and nasopharyngeal amyloidosis. 3,4
Clinical manifestations vary with hoarseness being the most frequent complaint on presentation. Other symptoms may be hemoptysis, dysphonia, dysphagia, or dyspnea in advanced disease. 5 Symptom severity varies depending on the location of the lesion. Most frequently involved are the ventricles, false vocal folds, true vocal folds, aryepiglottic folds, and the subglottis. 5
Computed tomography is a valuable imaging modality not to identify the nature of the lesion but in order to delineate the extent of the lesion. On magnetic resonance imaging, amyloid appears isointense to skeletal muscle and thus helps the clinician to differentiate it from malignancy. 2,5 The gold standard for the diagnosis is tissue biopsy and examination of the specimen stained with Congo red under a polarizing microscope, which shows characteristic apple green birefringence. 1
Several treatment methods have been proposed, ranging from observation to hemilaryngectomy. 5 Endoscopic excision with cold instruments and CO2 laser excision remain methods of choice. 2 The aim of every intervention in these cases is to provide a patent airway in combination with good voice quality. Long-term follow-up is of paramount importance so as to detect and treat possible recurrences. Very rarely, laryngeal amyloidosis progresses to systemic, but more than 50% of patients have local recurrence or multifocal local disease. 1
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.