
Abstract

Laryngotracheal stenosis (LTS) is a rare but well-described entity. Adult LTS is generally acquired secondary to iatrogenic airway manipulation, trauma, systemic disease, or idiopathic causes. 1,2 Prolonged intubation and tracheotomy are the primary etiologies of adult LTS. Although tracheotomy can reliably bypass LTS, the impact on patients’ quality of life is not insignificant. 3
Surgical management of LTS includes endoscopic procedures, open resection with anastomosis, or open reconstruction with expansion or grafting. 2 Endoscopic management with laser excision and dilation has gained favor as the initial treatment strategy. 4 We present a case of calcified subglottic stenosis, in which the novel application of an ultrasonic aspirator was required for successful resection.
A 68-year-old female presented for evaluation after unsuccessful intubation. The patient reported a history of mild asthma and a remote history of a motor vehicle accident requiring tracheotomy for 6 months. Pulmonary function tests (PFTs) showed a reduction in vital capacity, but no evidence of fixed obstruction. A limited view of the subglottis on flexible laryngoscopy revealed a transverse scar band. A neck computed tomography demonstrated irregularity of the posterior aspect of the subglottic trachea with areas of calcification (Figure 1).
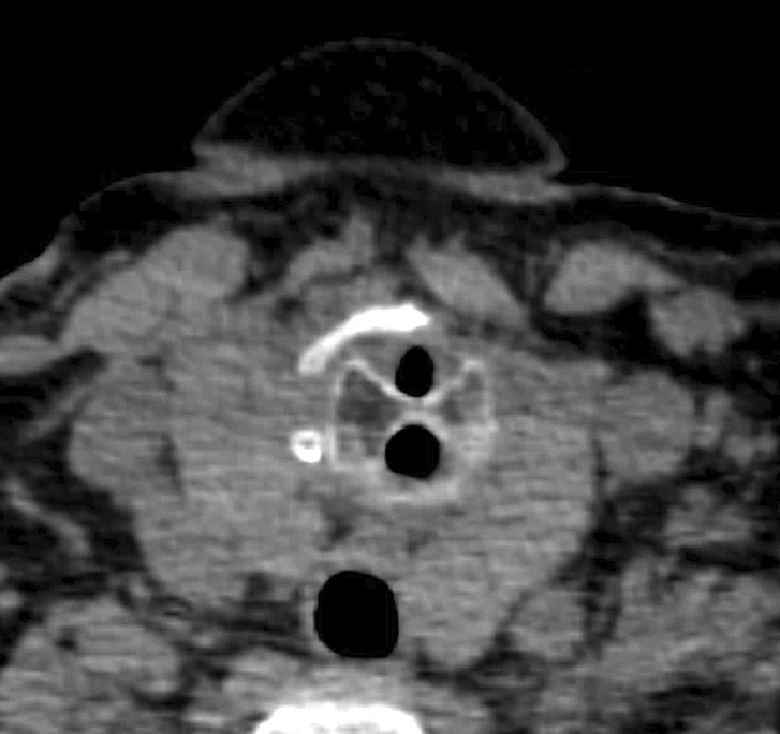
Axial computed tomography (CT) of the neck showing the calcified scar band extending within the airway creating 2 separate inlets.
During bronchoscopy, a transverse scar band was found immediately below the true vocal folds, with a 6 mm channel anteriorly and a 4 mm channel posteriorly (Figure 2A). There was a small anterior wall stenosis 3.0 to 3.7 cm below the true vocal folds at her prior tracheotomy site. The CO2 laser was used to make linear cuts in the anterior-posterior (AP) direction through the scar band with findings of underlying calcified tissue that could not be ablated effectively. A 1 mm Kerrison was used to divide the bone.
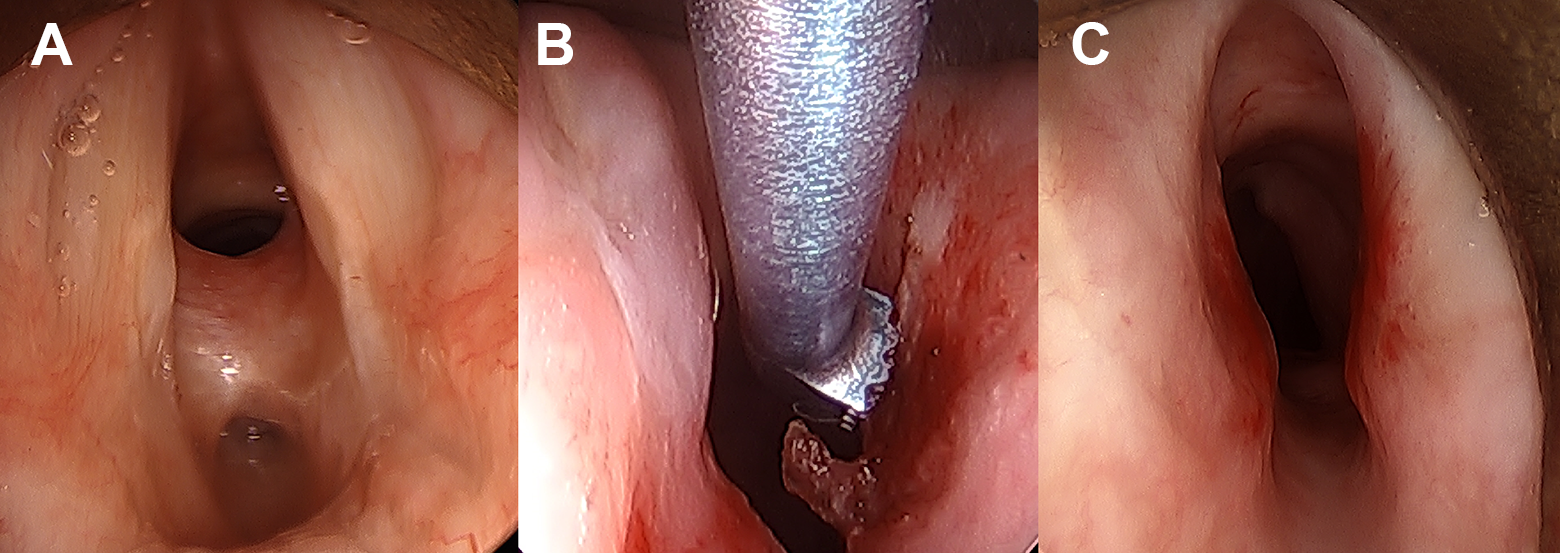
A, Intraoperative direct laryngoscopy view of calcified scar band. B, Intraoperative use of ultrasonic aspirator to remove stenosis. C, Follow-up Microdirect Laryngoscopy (MDL) after first-staged resection.
At follow-up, soft tissue scar had reformed across the bony bridge. She subsequently underwent 2-staged submucosal resections of the bony stenosis using an ultrasonic aspirator (Sonopet; Stryker, Kalamazoo, MI). Intraoperatively, a mucosal flap was elevated over the bony prominence of the stenosis. Using a 30° rod lens scope for visualization, the ultrasonic aspirator was used to remove the bony ledge (Figure 2B), resulting in a 5.0 MLT-sized airway (Figure 2C). The patient has remained asymptomatic with endoscopically confirmed airway patency without further dyspneic complaints or voice changes for the last 12 months.
The reported incidence of LTS after intubation ranges from 1% to 8.3%. 1,2 Composition of stenotic tissue is variable, with animal models showing temporal maturation from soft granulation tissue to mature, firm scar. 1 Calcification of subglottic stenosis is not documented extensively, but mineralization of soft tissue after trauma has been described in orthopedic literature. 5 In our patient, calcification of the mature scar band likely resulted via endochondral ossification driven by the intact adjacent perichondrium of the cricoid cartilage.
Endoscopic ablation of stenosis with CO2 laser is commonly used due to its shallow depth of penetration and minimal nonspecific thermal affect—a limitation for our resection. 2,4 Ultrasonic aspirators have been used in orthopedics, neurosurgery, and more recently in skull base surgery for their ability to remove bony tissue with minimal damage to adjacent tissue. 6 They utilize Piezoelectric principles to convert electrical energy to mechanical oscillations of a defined frequency, resulting in tissue removal by cavitation. 6 In our case, a hand piece with a unidirectional tip allowed for removal of the bony ledge without damaging the mucosal flap. The hand piece fit through a laryngoscope with an angled scope to optimize visualization. The novel application of this instrument allowed for the treatment of a subglottic scar band not amenable to previously described endoscopic resection techniques.
Footnotes
Authors’ Note
Presented at Combined Otolaryngology Spring Meeting, American Broncho-Esophagological Association; April 18-22, 2018; National Harbor, MD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.