
Abstract

Vocal fold nodules (VFNs) predominantly grow in women at the junction of the anterior and middle thirds of the vocal fold, where abusive phonation and/or intense cough cause the greatest injury to the mucosa. 1 They impose limitations on vocal. This results in dysphonia: hoarse and breathy voice, impaired vocal range, and pain during phonation, which is caused by compensatory hyperfunction. 2 Treatment is mostly conservative, with indications for endolaryngeal phonosurgery when there is no improvement. 3
A 36-year-old woman sought medical attention at our ENT outpatient department due to dysphonia and breathy voice for 18 months. There was no pain on phonation, but the symptoms were worsening. She had been working as a teacher for 12 years. The diagnosis of VFNs with severe voice impairment (Voice Handicap Index [VHI] score 63) had been established by a phoniatrician. There were indications for phonosurgery due to persistent symptoms following voice therapy and treatment with inhaled glucocorticosteroids. The patient also had a nodular goiter and was on a waiting list for thyroidectomy. The purpose of her consulting an ENT surgeon was to get an opinion regarding the necessity of undergoing phonosurgery for the VFNs before the thyroid surgery. Upon examination, typical bilateral, localized VFNs were seen endoscopically. The lesion on the right vocal fold was slightly smaller than the contralateral one (Figure 1A). The patient was advised to undergo thyroid surgery first and to return for an ENT examination in order to plan phonosurgery for the VFNs. Subsequently, thyroidectomy was performed under general anesthesia in another hospital. A cuffed 5.0-mm endotracheal tube was used for intubation with no difficulties encountered. Directly after the surgical procedure, the patient experienced sudden improvement in her voice quality. Normal vocal fold morphology and function with symmetrical mobility of the vocal folds and complete glottic closure were confirmed at our department 3 weeks later (Figure 1B). Her maximum phonation time was 23 seconds, and her VHI score was 22. She was referred to the voice therapy department in order to change her potentially inappropriate phonatory habits. The patient has also had ENT care for 18 months with no recurrence of symptoms or complaints.
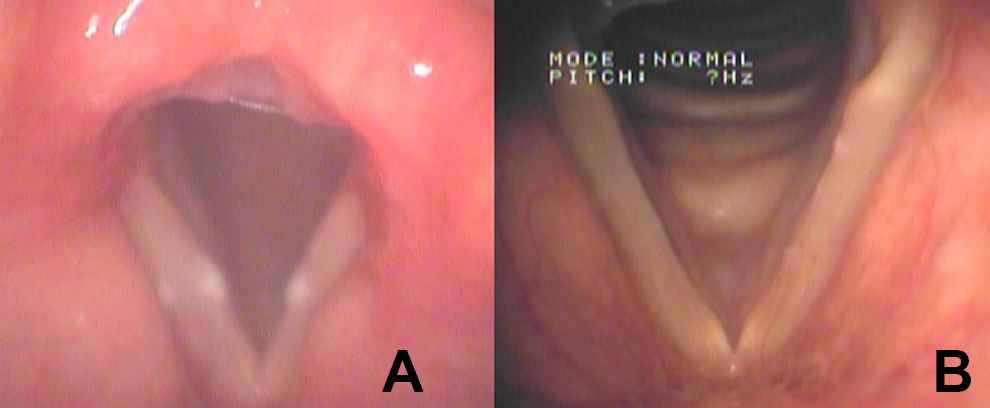
A, Bilateral vocal fold nodules at initial examination. B, The patient’s larynx 3 weeks after thyroid surgery.
A PubMed search did not retrieve reports of any cases of accidental VFN removal related to endotracheal intubation. On the contrary, fibrous VFN lesions resulting from endotracheal intubation in pediatric patients have been reported. 4 The VFNs in our patient could have been sheared off during intubation but were most likely removed during extubation. The removal of an incompletely deflated cuff might have been the reason for this accidentally beneficial event. 5 This hypothesis is much more probable than simultaneous removal of bilateral VFNs during endotracheal intubation which presented no difficulties. 6 There are many phonosurgical procedures for VFNs performed worldwide, 3 but no reports of VFN accidental removal during intubation have been published. The experience from this case suggests the need for great care in handling the intubation tube, particularly in patients with lesions localized on the free margins of the vocal folds. Although the consequences of endotracheal tube trauma were favorable in this unusual case, tube trauma causes dysphonia much more often than it cures it.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.