
Abstract

Physical examination is essential in the practice of medicine. Although the patient can tell us their subjective symptoms and complaints, it is up to the medical practitioner to recognize often subtle physical findings that will help to determine diagnosis, prognosis, and treatment. However, interpretation of physical findings can be rather subjective as they are often descriptive and can vary from individual to individual practitioner. Classification schemes can help elucidate such areas of confusion by defining set criteria for each class in the schema. With classification schemes, there may be less subjectivity when describing a physical finding.
In the field of laryngology, there have been multiple classification schemes of laryngeal findings based on pathology and observation, but few purely based on physical findings or phenomenology of laryngeal hyperadduction. An issue with all scales based on diagnoses and etiologies is that they can introduce a certain amount of bias as practitioners try to fit a physical finding into a classification scheme to fit into a diagnosis.
Laryngeal hyperadduction is one manifestation of laryngeal hyperfunctionality, which encompasses not just laryngeal hyperadduction but would include agonist/antagonist activity, for example, laryngeal tremor as well as other neurologic symptoms such as myoclonic jerks. One such proposed classification that includes only pure laryngeal hyperadduction and does not describe other types of laryngeal hyperfunctionality is one that Koufman proposed in 1991. 1 These other types of hyperfunctional manifestations may be seen, should be noted, and may be essential in diagnosis. They may also present in conjunction with laryngeal hyperadduction.
Hyperadduction can occur at multiple levels and can have very different physical presentations based on the hyperfunction of different groups of muscles, for example, contraction at the glottis compared to contraction at the supraglottis. Supraglottic hyperadduction is seen in a variety of vocal disorders ranging from Parkinson disease to spasmodic dysphonia. 2 Treatment may vary based on the location of contraction.
Morrison and Rammage described in 1993 a classification scheme for muscle misuse voice disorders. His classification scheme was based on the laryngeal isometric, glottis, and supraglottic lateral contraction states; anteroposterior contraction states; conversion aphonia; psychogenic bowing; and adolescent transitional dysphonia. 3 Although a good classification scheme, it is not purely phenomenologic and does not describe solely laryngeal hyperadduction.
Remacle et al in 2003 proposed a classification based on pathology and therapeutic aim. Vocal fold pathology that required phonosurgery were divided into 2 groups: one based on vocal fold lesions that impair vibratory movements requiring excision, incision and suction, dissection, coagulation, and so on, and another based on vocal fold movement disorders requiring position and/or tension correction by augmentation, injection, or excision. 4 The classification is based on treatment modalities and is excellent in describing which lesions need which therapeutic modality, but again is based more on pathology and treatment. It also does not describe laryngeal hyperadduction in pure phenomenologic terms.
Majdevac et al describes a classification of dysphonia based on the primary etiologic factor in 2 separate articles. These again are based on etiology/pathology and not on phenomenology. 5,6
Koufman et al in 1982 classified functional voice disorders into 5 types: type 1—hysterical aphonia, type 2—habituated hoarseness, type 3—falsetto voice, type 4—vocal abuse, and type 5—postoperative dysphonia. 7 The classification is a good description of various etiologies of functional voice disorders but again does not address phenomenology of laryngeal hyperadduction.
In 2001, Belafsky et al published a validated scoring index for reflux based on observations of inspection of the larynx, an excellent example of a phenomenological-based classification. 8 To our knowledge, the only classification scheme that defines the physical findings of laryngeal hyperadduction alone is the one proposed by Koufman in 1991. 1
Per Koufman description from 1991, type 1 hyperadduction would be defined as hyperadduction and contraction at the level of the vocal folds where the arytenoids become compressed in the lateral plane (Figure 1). Type 2 hyperadduction would be defined as hyperadduction at the level of the false folds where the false folds contract (Figure 2). Type 3 hyperadduction is defined as hyperadduction when the arytenoid makes contact with the petiole of the epiglottis (Figure 3). This contraction would be in an anterior–posterior plane compared to type 1 which is more in a lateral plane. Type 4 hyperadduction is defined as sphincteric closure of the supraglottis (Figure 4).
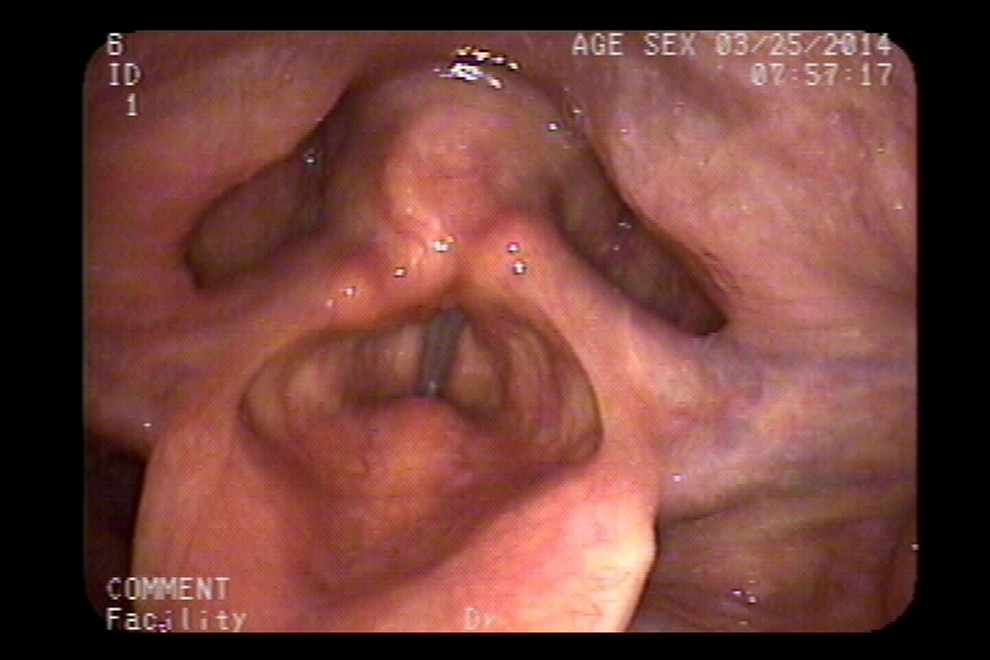
Type 1 hyperadduction would be defined as hyperadduction and contraction at the level of the vocal cords where the arytenoids become compressed in the lateral plane.
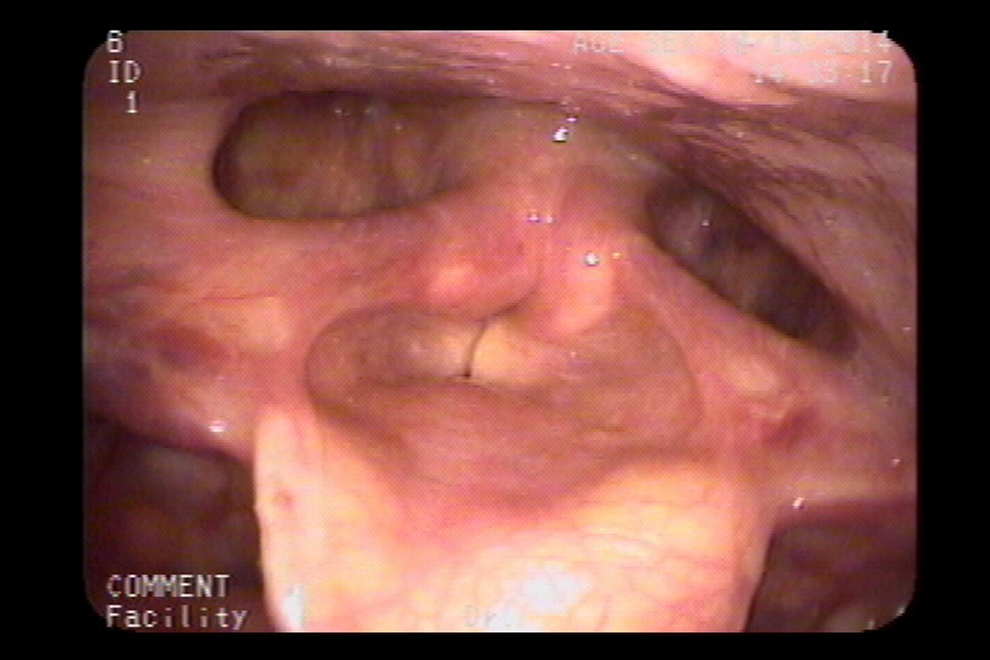
Type 2 hyperadduction would be defined as hyperadduction at the level of the false cords where the false cords contract.
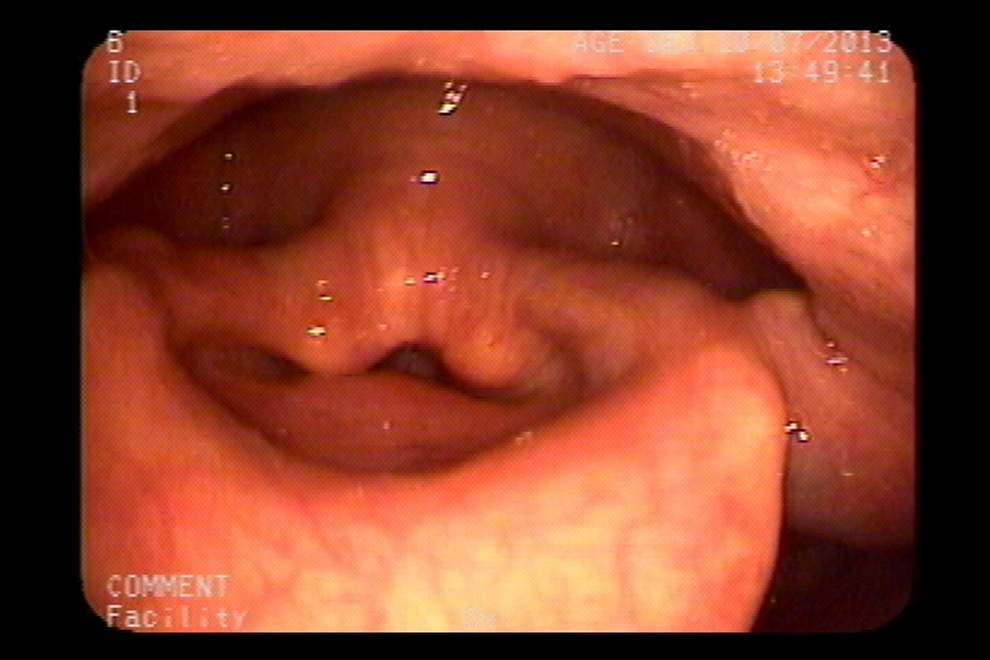
Type 3 hyperadduction is defined as hyperadduction when the arytenoid makes contact with the petiole of the epiglottis. This contraction would be in an anterior–posterior plane compared to type 1 which is more in a lateral plane.
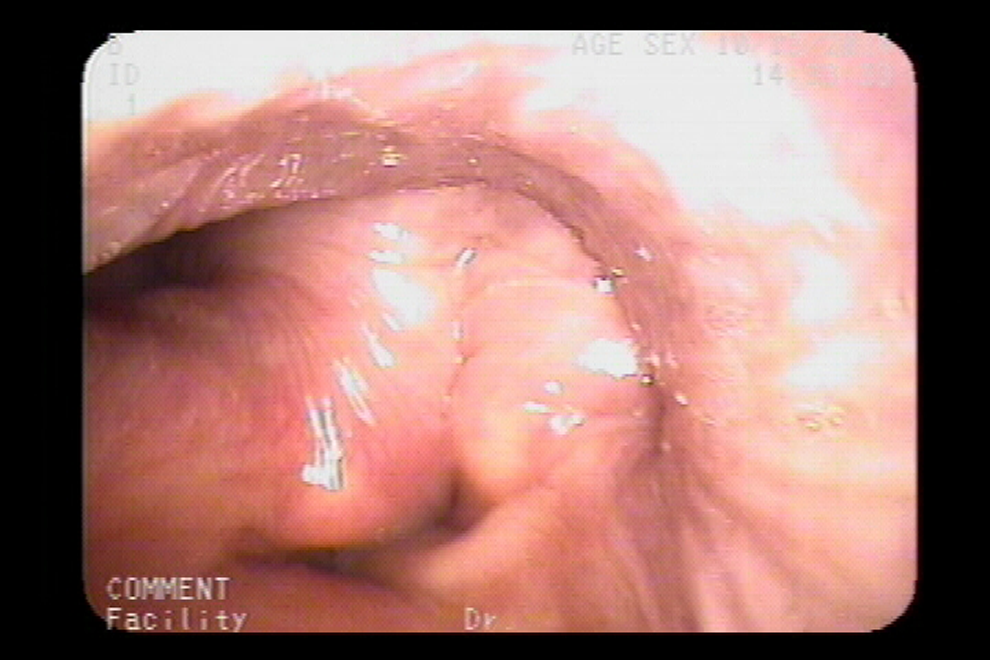
Type 4 hyperadduction is defined as sphincteric closure of the supraglottis.
A unique set of muscles affect each class of hyperadduction. In type 1 hyperadduction, the lateral cricoarytenoid and interarytenoid muscles are primarily responsible for hyperadduction at the level of the glottis. In type 2, there is contraction of the supraglottic musculature, including oblique fibers of the thyroarytenoid, in addition to those of type 1. In type 3 contraction, the muscles included are all of the above in addition to contributions from the thyroarytenoid. With type 4 contraction, there is mass muscle activity including the supraglottic musculature such as the aryepiglottic muscles resulting in sphincteric closure.
All of these types of hyperadduction can be seen in spasmodic dysphonia and muscle tension dysphonia as well as other hyperfunctional disorders. In patients with supraglottic squeeze, although most patients can have their supraglottis “unloaded” with intensive speech therapy, some patients continue to have supraglottic squeeze despite combined therapy. 9
As described earlier, this classification is based purely on hyperadductive phenomenology. Other types of laryngeal hyperfunction may not be described by these 4 classifications. For example, patients who have laryngeal tremor or myoclonic jerks may also have laryngeal hyperadduction at one or multiple levels, but may be difficult to place into a particular classification. These need to be taken into account when describing these phenomena.
Overall, Koufman’s classification of laryngeal hyperadduction is an excellent purely phenomenologic classification scheme and is a useful tool in describing this physical finding.
Footnotes
Authors’ Note
The principal investigator Christopher Tang had full access to all the data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis. Presented at the 2015 AAO-HNS meeting by the principal investigator Christopher Tang, MD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.