
Abstract

A 51-year-old female presented to the laryngology clinic for evaluation of a 1-year history of cough, worsened over the preceding month, as well as gradual onset of a foreign body sensation and hoarseness. She denied dysphagia, odynophagia, cervical mass, and a history of voice abuse. She reported previous treatment for laryngeal candidiasis and excision of a benign vocal fold lesion. Medical history was also significant for asthma treated with inhaled steroids and a hiatal hernia treated with fundoplication with persistent postoperative reflux. Laryngoscopy revealed a mass of granulation-like tissue arising from the posterior commissure without obstruction of the airway (Figure 1). Stroboscopy demonstrated normal vocal fold mobility and an intact mucosal wave. The remainder of the head and neck examination was unremarkable.
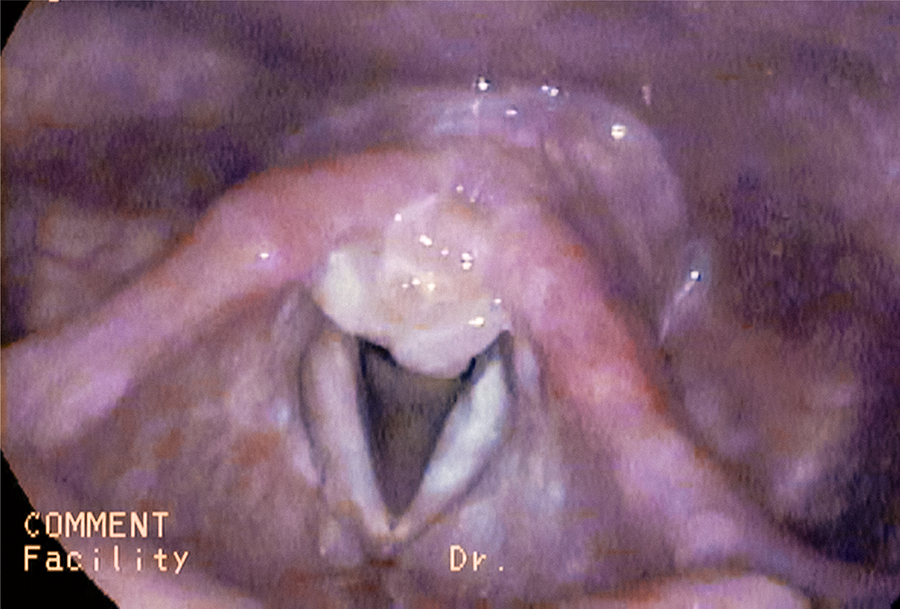
Mass of granulation-like tissue arising from the posterior commissure noted on initial flexible laryngoscopy.
Given the presence and persistence of a laryngeal mass despite an adequate regimen of reflux management, suspension microlaryngoscopy was undertaken for biopsy and excision. The mass was excised using cold steel technique, and the site of attachment of the lesion was injected with a corticosteroid. No other laryngeal abnormalities were noted. After recovery from surgery, the patient’s globus sensation and dysphonia resolved, and her cough significantly improved. Histopathologic examination of the specimen demonstrated an ulcerated lesion in the laryngeal mucosa (Figure 2) with numerous round fungal organisms identified within necrotic debris and highlighted by positive periodic acid–Schiff and mucicarmine staining. Based on these findings, the patient was diagnosed with a laryngeal cryptococcal infection. An infectious disease specialist further evaluated the patient with no other remarkable findings. She remained on oral antifungal therapy for 5 months with continued requirement for inhaled corticosteroid therapy. No evidence of recurrent laryngeal infection or lesion was noted on active surveillance 3 years after treatment.
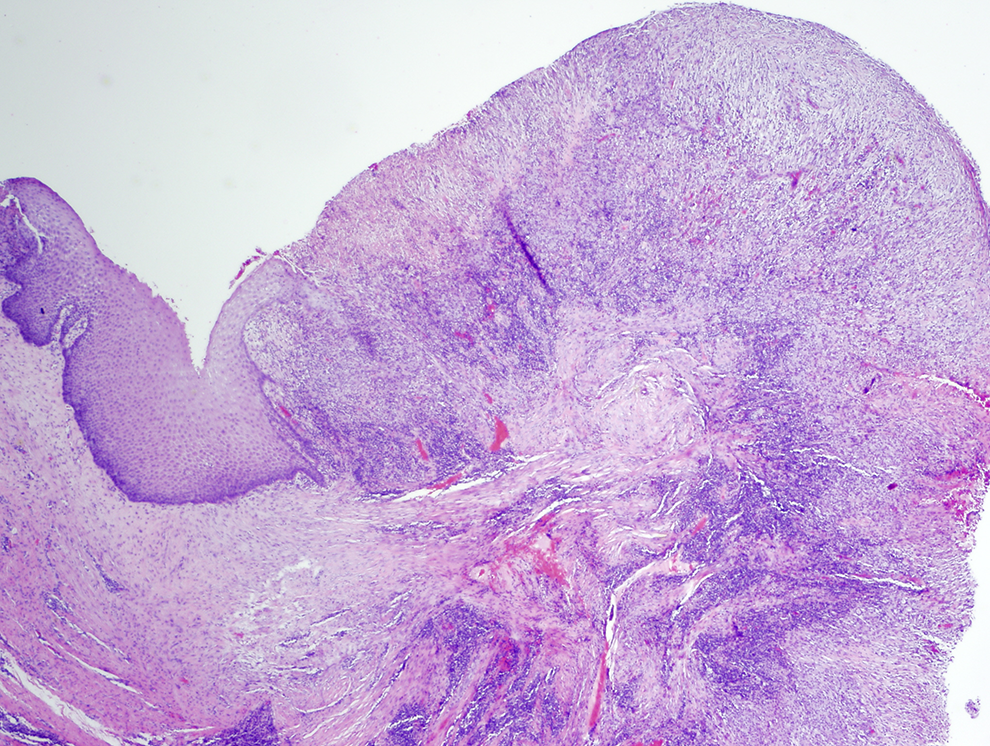
Low-power hematoxylin and eosin stain showing an ulcerated lesion in the laryngeal mucosa.
Cryptococcus is an opportunistic encapsulated species of yeast commonly found in soil, aged bird droppings, and decayed wood. 1 It is a common cause of pulmonary infection in immunocompromised patients, and it has the potential to disseminate to regions such as the central nervous system, meninges, bone, or subcutaneous tissue. In healthy patients, it may lead to a self-limited subacute infection. 2 It is thought that dissemination occurs via hematogenous spread from a primary focus, such as the lung, or from direct implantation by inhaled aerosolized organisms. 3 Laryngeal infection with Cryptococcus is rarely identified as a cause of hoarseness with the literature limited to case reports. 4,5 A high clinical suspicion followed by microlaryngoscopy and tissue biopsy are necessary for diagnosis, with special stains needed to detect fungal elements. A variety of nonspecific findings can be seen on physical examination including leukoplakia, laryngeal edema, vocal fold erythema, or a vocal fold mass or irregularity. It is important to rule out other, more common, laryngeal pathology such vocal fold cysts or polyps, papilloma, premalignant lesions, and malignant tumors. Measurement of cryptococcal antigen may be useful as a diagnostic and monitoring adjunct but has not been validated for use in isolated laryngeal disease. 4,6 Prolonged inhaled corticosteroid therapy in immunocompetent patients has been identified as a major risk factor for laryngeal cryptococcosis. 4 Other possible risks include tobacco use, exposure to chicken manure, mycobacterial infection, oral corticosteroid use, HIV infection, hepatitis C infection, diabetes mellitus, and previous cryptococcal pneumonia. 6
Given the rarity of laryngeal cryptococcosis, there are no evidence-based guidelines for management. The Infectious Diseases Society of America provides guidelines for the management of cryptococcal infection but does not specifically address laryngeal involvement. Antifungal therapy with oral fluconazole (400 mg daily) is the mainstay of treatment, and consultation with an infectious disease specialist is advised. 7 Suggested duration of antifungal therapy varies in the literature and has been reported between 4 weeks and 10 months. At least 6 weeks of therapy are recommended. Discontinuation or modification of inhaled corticosteroids should be considered, if possible. 4,8 Endoscopic excision in selected cases, and pulse dye or potassium titanyl phosphate (KTP) laser to treat fungal lesions have been described as adjuncts to management. 5,9
Laryngeal cryptococcosis remains a rare cause of hoarseness. A high degree of clinical suspicion is warranted, particularly in patients using an inhaled corticosteroid. The diagnosis is confirmed with biopsy and fungal stains. A course of oral antifungal therapy of adequate duration is the mainstay of therapy, with surgical intervention as an adjunct. Surveillance to resolution and comanagement with an infectious disease consultant are recommended.
Footnotes
Authors’ Note
The views expressed in this article are those of the author(s) and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government. The authors are military service members. This work was prepared as part of their official duties. Title 17 U.S.C. 105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. 101 defines a US Government work as a work prepared by a military service member or employee of the US Government as part of that person’s official duties.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.