
Abstract
A 48-year-old woman presented with a history of fever, oral malodor, sore throat, and left-sided otalgia for 6 days. She was diagnosed with an upper respiratory infection and was empirically treated with amoxicillin–clavulanate for 5 days by her family physician. Thereafter, she presented to our outpatient clinic due to her persistent symptoms despite the prescribed treatment of antibiotics. She indicated no history of trauma, surgery, foreign body, or medical illness.
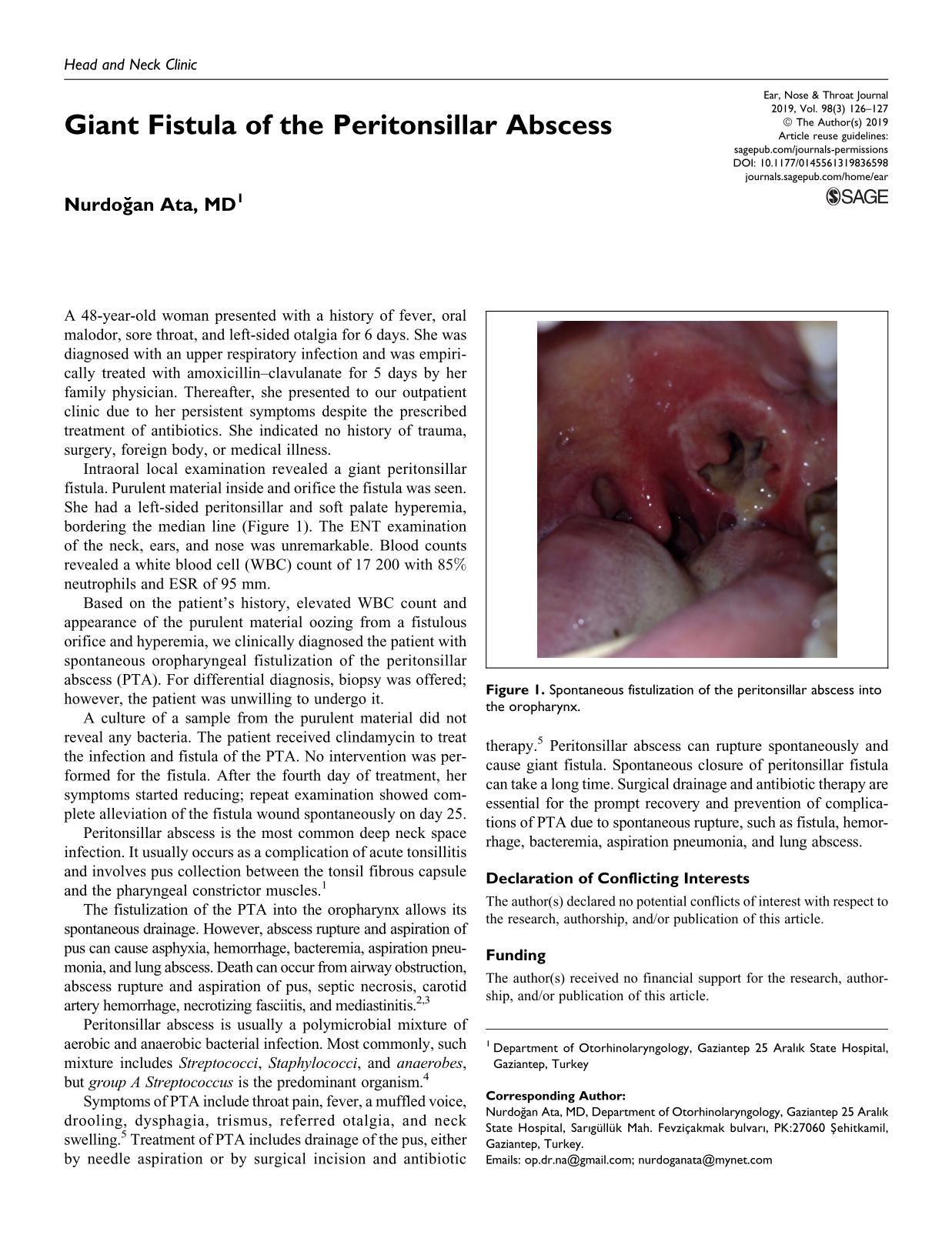
Intraoral local examination revealed a giant peritonsillar fistula. Purulent material inside and orifice the fistula was seen. She had a left-sided peritonsillar and soft palate hyperemia, bordering the median line (Figure 1). The ENT examination of the neck, ears, and nose was unremarkable. Blood counts revealed a white blood cell (WBC) count of 17 200 with 85% neutrophils and ESR of 95 mm.

Spontaneous fistulization of the peritonsillar abscess into the oropharynx.
Based on the patient’s history, elevated WBC count and appearance of the purulent material oozing from a fistulous orifice and hyperemia, we clinically diagnosed the patient with spontaneous oropharyngeal fistulization of the peritonsillar abscess (PTA). For differential diagnosis, biopsy was offered; however, the patient was unwilling to undergo it.
A culture of a sample from the purulent material did not reveal any bacteria. The patient received clindamycin to treat the infection and fistula of the PTA. No intervention was performed for the fistula. After the fourth day of treatment, her symptoms started reducing; repeat examination showed complete alleviation of the fistula wound spontaneously on day 25.
Peritonsillar abscess is the most common deep neck space infection. It usually occurs as a complication of acute tonsillitis and involves pus collection between the tonsil fibrous capsule and the pharyngeal constrictor muscles. 1
The fistulization of the PTA into the oropharynx allows its spontaneous drainage. However, abscess rupture and aspiration of pus can cause asphyxia, hemorrhage, bacteremia, aspiration pneumonia, and lung abscess. Death can occur from airway obstruction, abscess rupture and aspiration of pus, septic necrosis, carotid artery hemorrhage, necrotizing fasciitis, and mediastinitis. 2,3
Peritonsillar abscess is usually a polymicrobial mixture of aerobic and anaerobic bacterial infection. Most commonly, such mixture includes Streptococci, Staphylococci, and anaerobes, but group A Streptococcus is the predominant organism. 4
Symptoms of PTA include throat pain, fever, a muffled voice, drooling, dysphagia, trismus, referred otalgia, and neck swelling. 5 Treatment of PTA includes drainage of the pus, either by needle aspiration or by surgical incision and antibiotic therapy. 5 Peritonsillar abscess can rupture spontaneously and cause giant fistula. Spontaneous closure of peritonsillar fistula can take a long time. Surgical drainage and antibiotic therapy are essential for the prompt recovery and prevention of complications of PTA due to spontaneous rupture, such as fistula, hemorrhage, bacteremia, aspiration pneumonia, and lung abscess.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.