
Abstract

Case Report
A 12-month-old female presented to the emergency department after falling from her 5-year-old sibling’s arms onto a blunt tipped pen he was simultaneously holding. She was neurologically intact and clinically stable on arrival. Physical examination was unremarkable aside from a 2-cm laceration in the soft palate without foreign body (FB) visualized on deep exploration. Endoscopy of bilateral nares, nasopharynx, and upper airway was also negative for abnormalities. Lateral neck X-ray demonstrated the pen tip over the right posterior nasopharynx embedded in adenoidal tissue. The patient underwent an extensive soft palate and nasopharyngeal exploration, including partial adenoidectomy under anesthesia that were again unrevealing for an FB. The decision to undergo computed tomography (CT) and CT angiogram (CTA) of the head was made and revealed the FB abutting the right carotid canal in the petrous apex (Figure 1). However, due to significant artifact, vascular injury could not be excluded.
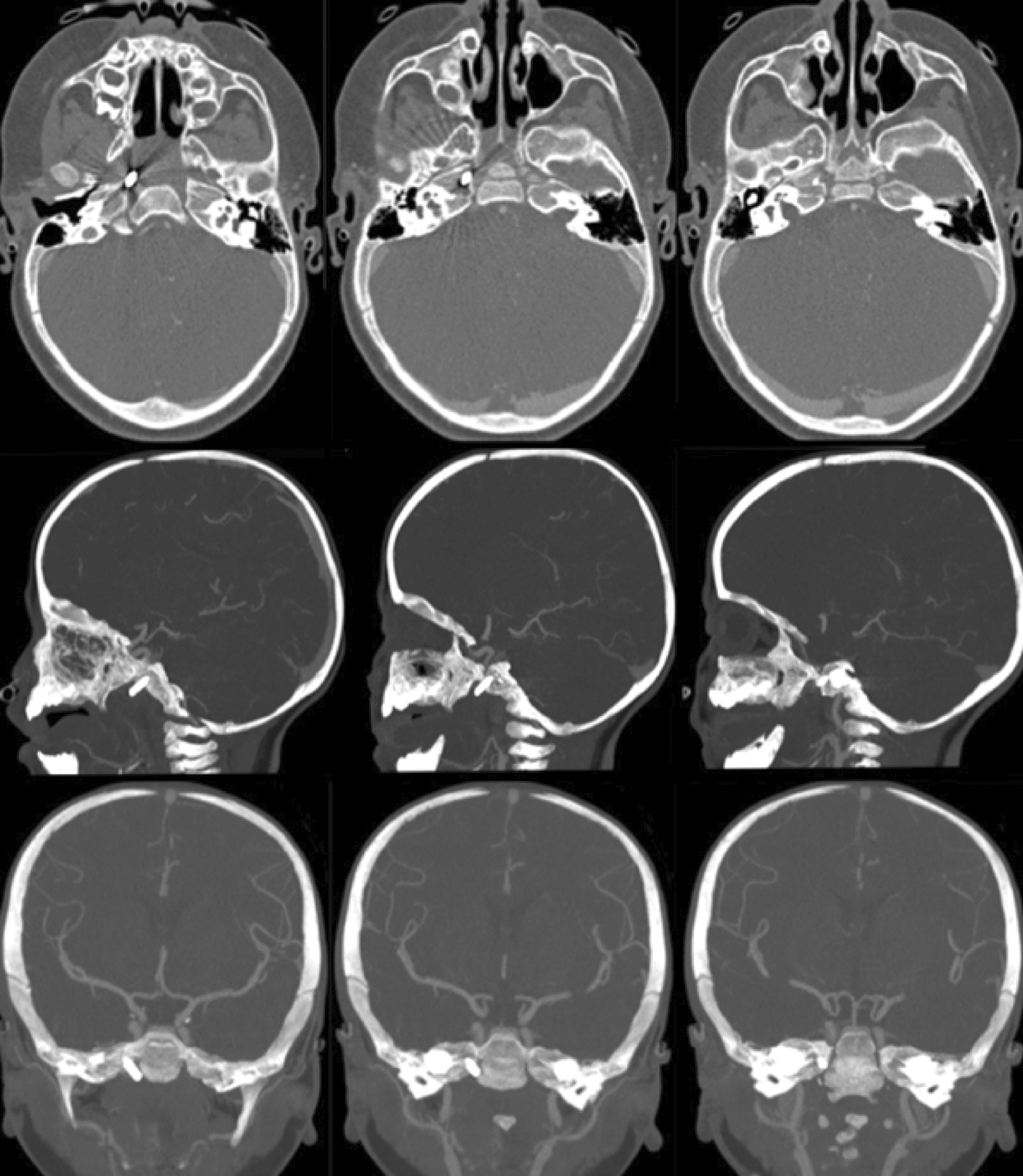
Computed tomography angiogram (CTA) demonstrating the trajectory and posterior extension of the metallic foreign body to the region of the right petrous apex, extending through the carotid canal.
Careful management and approach to her FB removal was planned among a multidisciplinary team including neurosurgery, interventional neuroradiology, skull-based rhinology, pediatric otolaryngology, and anesthesiology while the patient was placed on prophylactic antibiotics.
Planned diagnostic cerebral angiogram with removal of the pen tip demonstrated a normal right internal carotid artery without evidence of injury, dissection, or pseudoaneurysm (Figure 2). Angiography of the cranial region revealed no evidence of the FB. Subsequent investigation identified a metallic object at the level of the gastroesophageal junction, suggesting dislodgement of the FB from the skull base confirmed by portable chest X-ray (Figure 3). A team consensus for no further intervention was concluded and the patient was extubated and monitored without complications before discharge home.

Cerebral angiography demonstrating a patent right carotid artery and cerebral vascular with no evidence of disruption, aneurysm, or dissection.

Portable chest X-ray demonstrating a radiopaque foreign body at the level of the gastroesophageal (GE) junction.
Discussion
Transoral blunt cerebrovascular injuries (BCVI) are rare and account for only 0.2% to 2.7% of blunt trauma incidents but are associated with fatal complications, including carotid trauma or thrombosis, intracranial injuries, mediastinitis, and airway obstruction. 1 –5 Subtle injuries may be overlooked for reasons including parental removal of the FB, lack of witness to the event, and incomplete history. 6 Children less than 2 years of age are particularly vulnerable to neurological injury due to incomplete ossification of the skull, allowing even small forces to penetrate through the skull and dura. 2 Therefore, a timely diagnosis and proper surgical management via a multidisciplinary approach are essential to achieve the most favorable outcomes. 7
High-resolution, thin-slice CT scans are the gold standard for evaluation of the bony skull base in blunt traumatic cases. 8 The Denver Criteria of BCVI screens patients based on signs and symptoms of BCVI to reduce radiation exposure and improve cost-effectiveness before screening with CTAs. 4,9 Although useful, the tool still has imperfections. Franz et al found 20% to 22% of trauma patients to have BCVI despite a negative screening. 10 The Biffl Scale or Denver Scale was developed to grade the extent of BCVI and provides practitioners with prognostic and therapeutic implications. 11 Our patient sustained a grade I versus II injury, inconclusive because of significant artifact. Thereby management was divided by the observational approach commonly taken for grade I injuries or the need for cerebral angiography and surgical removal. When assessment for cerebral vascular injury is equivocal on CTA, catheter-based angiography is recommended to rule out dissection or pseudoaneurysm. 12 Retainment of the FB and risk for intracranial infection or erosion into surrounding structures was the determining factor in moving forth with surgical management.
Anesthetic considerations for FB involvement of the carotid sheath are numerous and critical. General anesthesia, large bore peripheral or central intravenous (IV) access, and placement of an arterial line are essential in the event of vascular injury where massive blood loss and hypotension can occur. Alternatively, arterial access obtained by the interventional radiologist may be used to transduce the arterial pressure, depending on the size of the sheath that is placed. Anesthesia appropriately managed IV access with use of two 24 g peripheral IVs for induction and placement of an airway before 2 additional larger bore IVs and an arterial line were placed.
Diagnostic angiography and balloon catheterization was planned to commence the procedure. Our skull-based rhinologist planned for nasal endoscopic removal using neuronavigation image guidance once the balloon was cannulated up through the tenuous area of the carotid. Sufficient collateral circulation was confirmed on initial CTA. In the event of hemorrhage or vascular compromise, the balloon would be deployed to tamponade any bleeding prior to arterial coiling.
Developing a strategic algorithm that provides a stepwise blueprint for management and anticipation of complications is critical in BCVI patients with retained FBs. A multidisciplinary team facilitates optimal surgical planning in anticipation for all possible complications to ensure successful outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.