
Abstract

A 89-year-old male patient with a 2-month history of unilateral nasal obstruction was referred to the Department of Head and Neck Surgery at our hospital. The patient’s past medical history provided significant information, including details of a 15 pack–year history of smoking, as well as a 3-year history of stage III hypertension and stage C heart failure (according to American Heart Association classification). On the surface, the patient showed no indication of any neuroendocrine neoplasms (NENs); he had no epistaxis, reported no headaches, there was no evidence of cervical lymphadenopathy and the cranial nerve examination at presentation was normal.
When a nasal endoscopy was performed, it was then discovered that a large nasopharyngeal mass, covered by normal mucosa, was obstructed the nasopharyngeal space (Figure 1). A biopsy was performed, and histology results showed uniform tumor cells with round nuclei and typical salt-and-pepper chromatin. Meanwhile, no pleomorphism or necrosis was observed the histology samples (Figure 2) and mitotic activity was quite low (less than 2 mitotic units per mm2). Moreover, immunohistochemical staining showed positive results for chromogranin, synaptophysin, nonspecific esterases (NSEs), CD56, and S-100 (Figure 3). The final diagnosis was made to a typical carcinoid and this was confirmed by at least 2 pathologists at our institution.
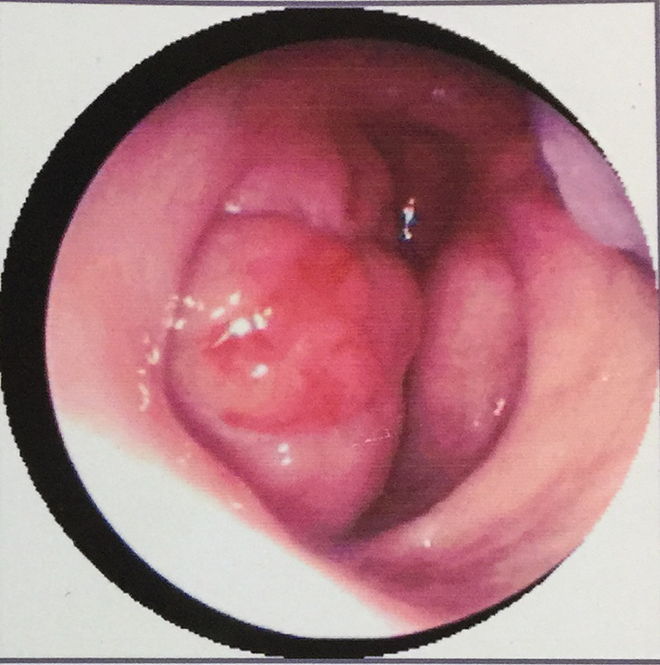
Nasal endoscopy revealed a large nasopharyngeal mass.
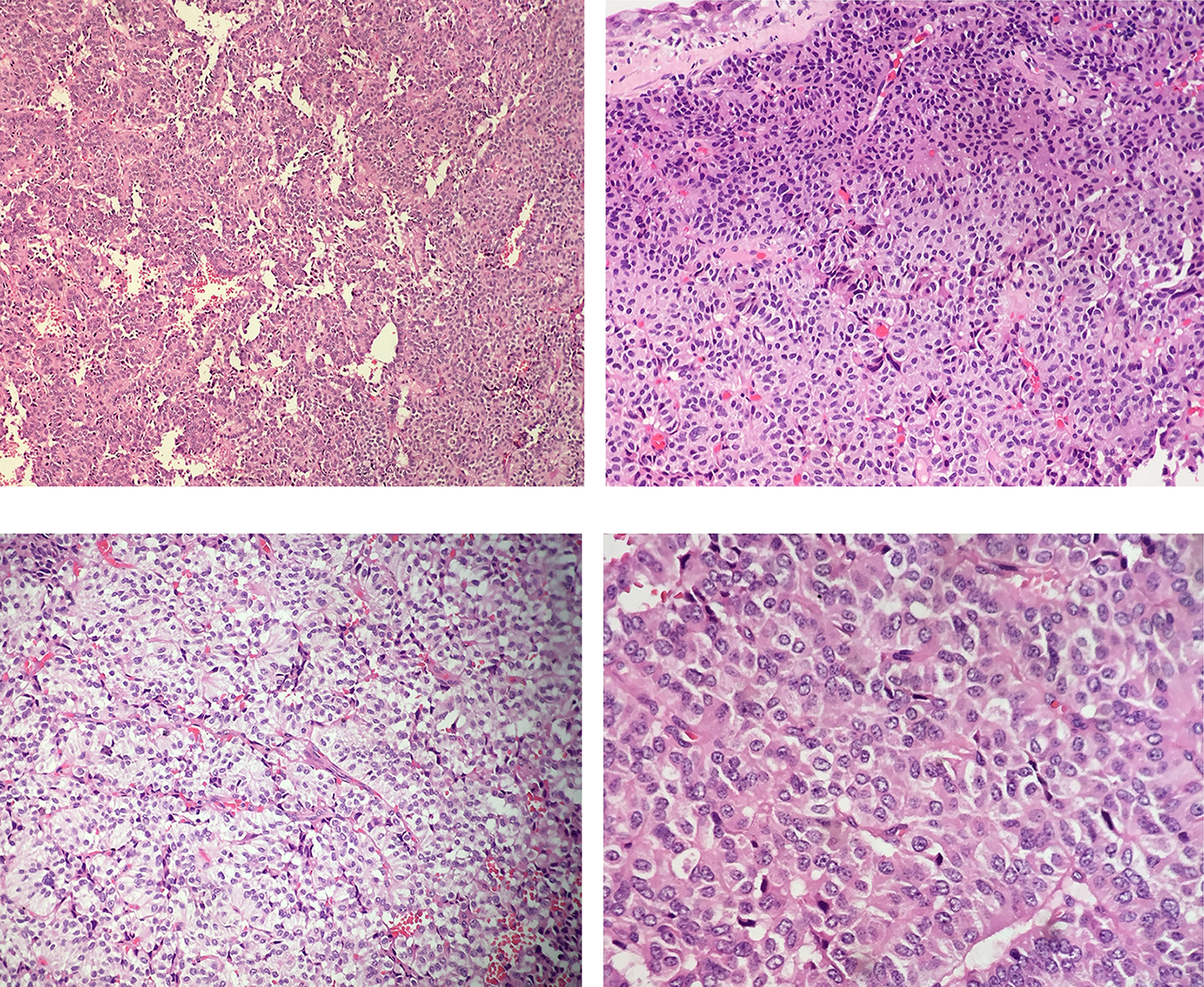
HE staining showed tissue containing uniform distribution of tumor cells with round nuclei and typical salt-and-pepper chromatin. Mitotic activity was low (less than 2 mitotic units per mm2), and there were no indications of pleomorphism or necrosis. HE indicates hematoxylin and eosin.
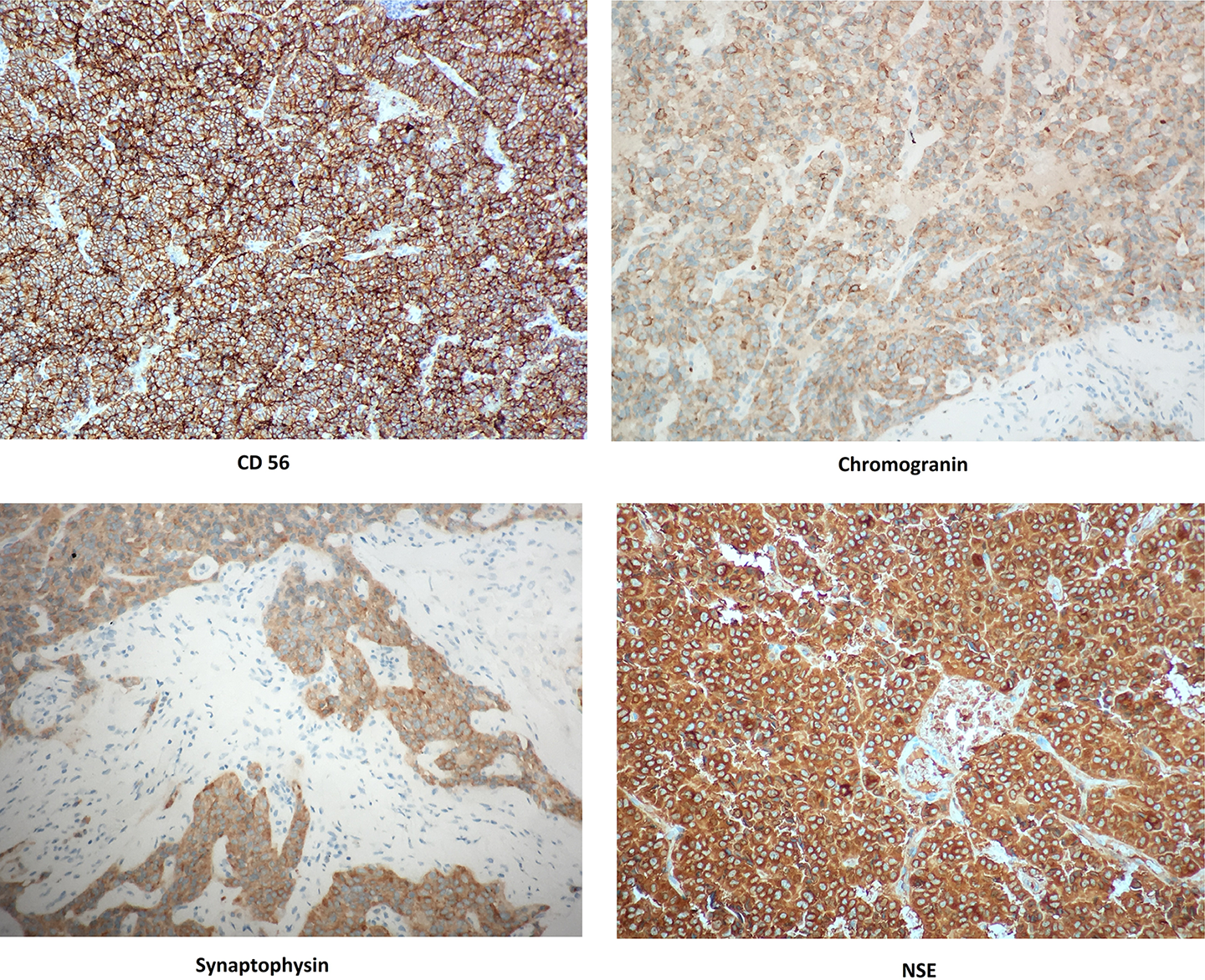
Immunohistochemical staining gave positive results for chromogranin, synaptophysin, nonspecific esterases (NSEs), and CD56.
Unfortunately, due to the patient history of severe heart failure and hypertension, the patient had denied treatment for the nasopharyngeal neuroendocrine tumor and died of heart failure after 5 months from initial diagnosis.
The World Health Organization’s classification system for NENs of the nasopharynx separates tumors into 3 major categories: typical carcinoids (well differentiated), atypical carcinoids (moderate differentiated), and small-cell carcinomas (poorly differentiated neuroendocrine carcinomas). 1
Primary carcinoid tumors of the head and neck are extremely rare and are found most commonly in the larynx, accounting for less than 1% of laryngeal tumors. 2,3 Neuroendocrine neoplasms of the nasopharynx are poorly understood, and to the best of our knowledge, only 3 other cases have been reported on typical carcinoid of the nasopharynx. 4 -6
Nasopharyngeal neuroendocrine carcinomas have histologic features similar to any other neuroendocrine carcinomas of any other primary origin site. 1 The diagnosis of a typical carcinoid tumor was made based on these histopathological results.
When a tumor is large and extensive, it is difficult to recognize its exact source, for example, whether it originates from the nasopharynx or the nasal cavity, and in these circumstances, a neuroendocrine tumor needs to be classified from other tumors, such as neuroendocrine carcinomas and olfactory neuroblastomas. Neuroendocrine carcinomas have been reported to stain immunohistochemically positive for chromogranin A, NSE, synaptophysin, neural-cell adhesion molecules (CD56), and AE1/AE3. 7,8 Immunostaining for S-100 protein has been reported positive in olfactory neuroblastomas and negative in neuroendocrine carcinomas, and this is often considered to be a key difference to determine the classification of the tumor. 9 In these situations, pathologists should make decisions based on both histological characteristics and immunohistochemical features for the differential diagnosis of neuroendocrine tumors.
In view of the small number of cases, a standard procedure for the successful treatment for a typical carcinoid tumor of the nasopharynx has yet to be established. The treatment of choice for a patient who has a localized typical carcinoid tumor is usually surgery. Radiotherapy and chemotherapy have been used in 3 previous cases, but the efficacy of those treatments is yet unclear. 4 -6
Typical carcinoid tumors occur rarely in the head and neck area. To the best of our knowledge, this was the fourth case with a typical carcinoid in the nasopharynx reported in published literature. A procedure for the successful treatment of carcinoids of nasopharynx has yet to be established; however, surgery seems to show promising results. In general, the prognosis for the treatment of a well-differential neuroendocrine tumor is to resect the tumor completely. Unfortunately, due to our patient’s old age and history of medical complications, we were not able to treat the tumor and determine a successful prognosis for the disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.