
Abstract
Case Presentation
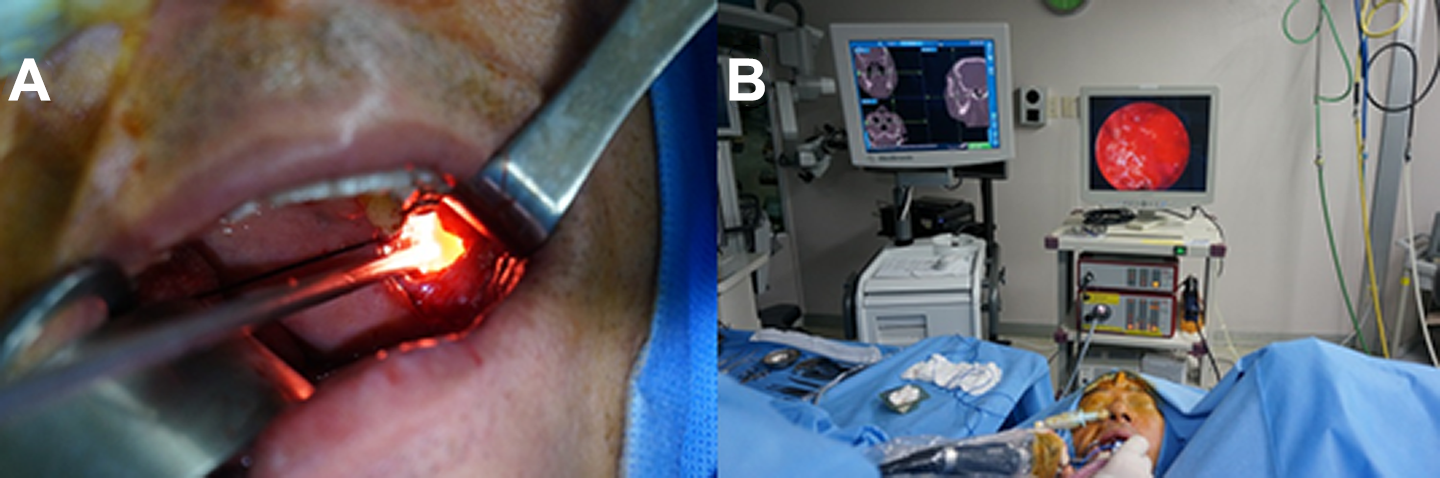
A 62-year-old man presented with a mass lesion of the left mandibular ramus and coronoid process, confirmed by facial bone computed tomography (CT). Facial bone CT revealed a well-defined 52.5 × 50.6 × 29.0 mm cystic lesion involving the left mandibular ramus and coronoid process. The adjacent bony structure was severely thinned and eroded, and the lining of the bone showed partial discontinuity (Figure 1).

Facial bone CT and 3D reconstruction images before surgery. A and B, A 52.5 × 50.6 × 29.0 mm sized well-defined, cystic lesion with low density involves left mandibular ramus and coronoid process. C, Adjacent bony structure is severely thinned and eroded. Three-dimensional reconstruction image shows the features documented above. CT indicates computed tomography; 3D, 3-dimensional.
Considering the findings described above, under suspicion of odontogenic keratocyst (OKC) of the mandible, navigation system–assisted endoscopic enucleation and chemical ablation was chosen as the treatment strategy.
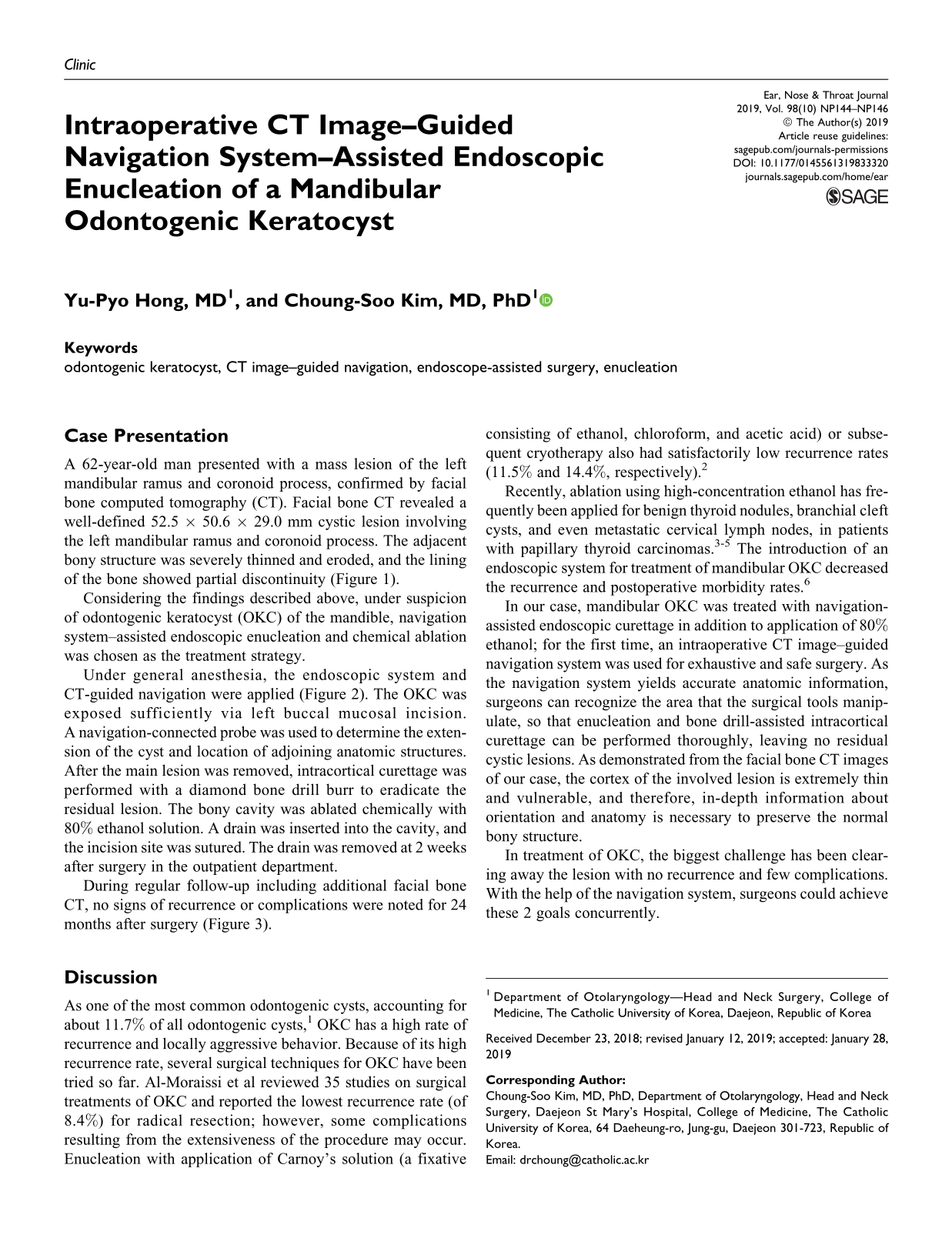
Under general anesthesia, the endoscopic system and CT-guided navigation were applied (Figure 2). The OKC was exposed sufficiently via left buccal mucosal incision. A navigation-connected probe was used to determine the extension of the cyst and location of adjoining anatomic structures. After the main lesion was removed, intracortical curettage was performed with a diamond bone drill burr to eradicate the residual lesion. The bony cavity was ablated chemically with 80% ethanol solution. A drain was inserted into the cavity, and the incision site was sutured. The drain was removed at 2 weeks after surgery in the outpatient department.
A, Intraoral approach for OKC. B, Navigation and endoscopic system indicate accurate anatomic information. OKC indicates odontogenic keratocyst.
During regular follow-up including additional facial bone CT, no signs of recurrence or complications were noted for 24 months after surgery (Figure 3).
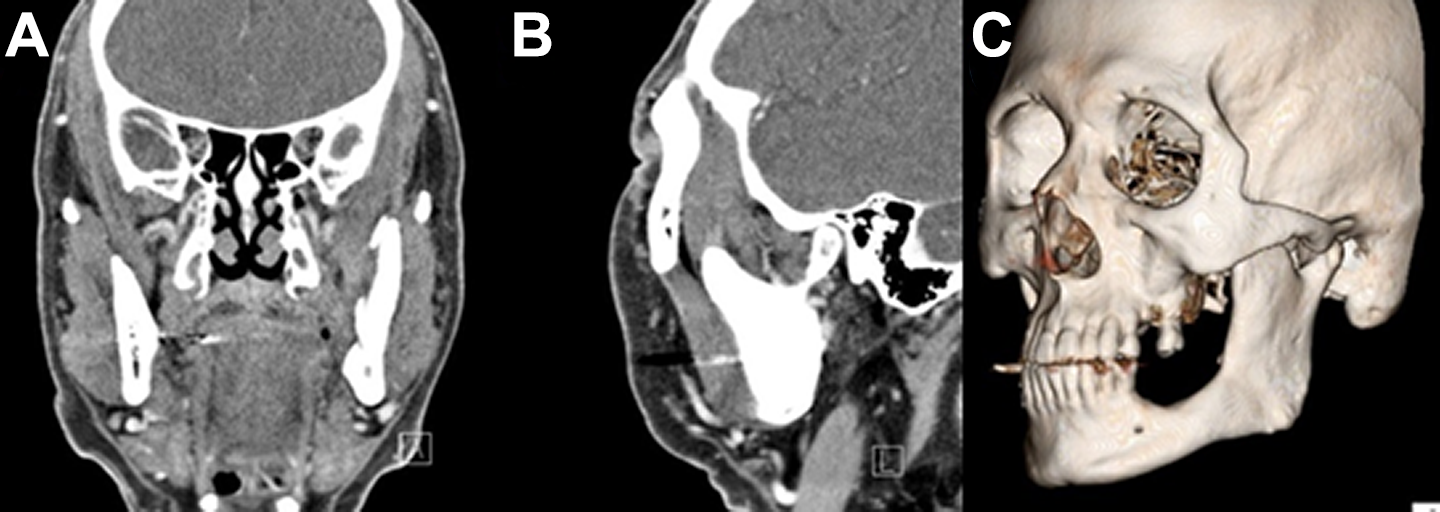
Facial bone CT and 3D reconstruction images 2 years after surgery. Bony structure of eroded mandibular ramus and coronoid process is regenerated and there is no evidence of recurrence. CT indicates computed tomography; 3D, three dimensional.
Discussion
As one of the most common odontogenic cysts, accounting for about 11.7% of all odontogenic cysts, 1 OKC has a high rate of recurrence and locally aggressive behavior. Because of its high recurrence rate, several surgical techniques for OKC have been tried so far. Al-Moraissi et al reviewed 35 studies on surgical treatments of OKC and reported the lowest recurrence rate (of 8.4%) for radical resection; however, some complications resulting from the extensiveness of the procedure may occur. Enucleation with application of Carnoy’s solution (a fixative consisting of ethanol, chloroform, and acetic acid) or subsequent cryotherapy also had satisfactorily low recurrence rates (11.5% and 14.4%, respectively). 2
Recently, ablation using high-concentration ethanol has frequently been applied for benign thyroid nodules, branchial cleft cysts, and even metastatic cervical lymph nodes, in patients with papillary thyroid carcinomas. 3 –5 The introduction of an endoscopic system for treatment of mandibular OKC decreased the recurrence and postoperative morbidity rates. 6
In our case, mandibular OKC was treated with navigation-assisted endoscopic curettage in addition to application of 80% ethanol; for the first time, an intraoperative CT image–guided navigation system was used for exhaustive and safe surgery. As the navigation system yields accurate anatomic information, surgeons can recognize the area that the surgical tools manipulate, so that enucleation and bone drill-assisted intracortical curettage can be performed thoroughly, leaving no residual cystic lesions. As demonstrated from the facial bone CT images of our case, the cortex of the involved lesion is extremely thin and vulnerable, and therefore, in-depth information about orientation and anatomy is necessary to preserve the normal bony structure.
In treatment of OKC, the biggest challenge has been clearing away the lesion with no recurrence and few complications. With the help of the navigation system, surgeons could achieve these 2 goals concurrently.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.