
Abstract

A 77-year-old female with a past medical history of rheumatoid arthritis (RA) requiring immunosuppression with methotrexate and abatacept over the last several months presented with a 4-week history of painful lesions on her left ear which evolved over several days into swollen, black eschars, and shallow ulcerations. She was urgently referred to our institution when outside pathology demonstrated an angioinvasive Fusarium fungal skin infection. Examination of the left ear revealed several serpiginous black necrotic eschars largely involving the antihelix as well as multiple other lesions involving the tragus, antitragus, and lobule (Figure 1). Written informed consent was obtained by the patient to obtain photographic evidence and to report her case. The largest lesion measured 2 cm × 1.5 cm. Laboratory work consisted of a white blood cell count of 6.22 k/mm3, erythrocyte sedimentation rate (ESR) of 10 mm/h, and C-reactive protein (CRP) of 0.19 mg/dL. A computed tomography of the temporal bone was negative for involvement of the mastoid.

Left ear fungal infection with shallow ulcerations and eschars.
She was brought into the operating room for debridement urgently due to concern for potential rapid progression of this infection, similar to the often-deadly disease process of acute invasive fungal rhinosinusitis. Lesions involving the lobule, tragus, antitragus, helix, antihelix, and root of the helix were excised until bleeding, viable tissue was encountered. All excised lesions were sent to the pathology department for histologic evaluation and tissue culture. Postoperatively, our infectious disease consultant recommended the patient start voriconazole 200 mg orally every 12 hours for the biopsy-proven Fusarium skin infection with angioinvasion. Histologic evaluation of the left ear lesion demonstrated marked necrosis of skin with extension into underlying cartilage. A Grocott-Gomori's Methenamine-Silver stain highlighted numerous septate fungal organisms within necrotic tissue with focal invasion into cartilage (Figure 2). Organisms were identified within blood vessels (Figure 3).

Grocott–Gomori’s methenamine silver (GMS) stain 200×—Fungal organisms with invasion into cartilage.
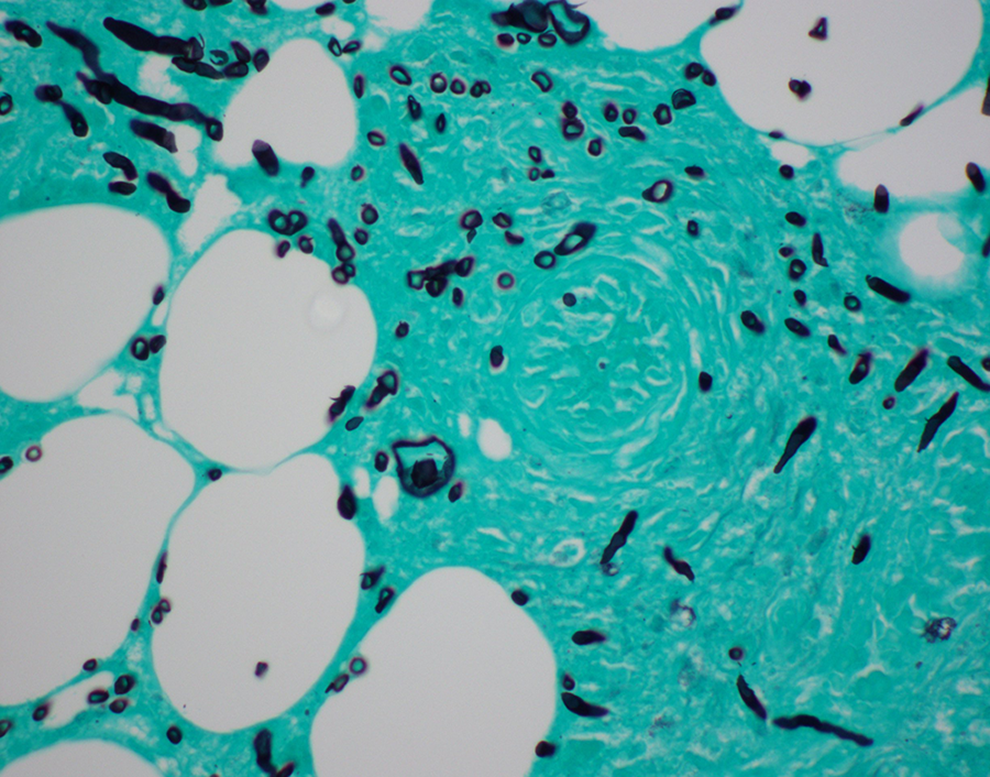
GMS stain 600×—Fungal organism within small artery (center).
Microbiology cultures of the lesion grew Stenotrophomonas maltophilia, Pseudomonas aeruginosa, Fusarium, and few Curvularia species. She was started on levofloxacin 750 mg orally daily for adequate coverage of the bacterial component. Blood cultures remained negative throughout her hospital stay. On postoperative day 4, the auricle was reconstructed with a full-thickness skin graft from the left supraclavicular fossa to provide coverage of the areas of exposed cartilage of the left ear. She was discharged on postoperative day 5 with a regimen of levofloxacin 750 mg orally total daily for 30 days and voriconazole 200 mg orally every 12 hours for 30 days in addition to her medications for RA. At her 6-week follow-up, she had no signs of infection or cartilage exposure.
Cutaneus angioinvasive fungal infections are extremely rare and based on a literature search, this appears to be the first report of a cutaneous, angioinvasive, and fungal infection of the auricle. Patients with RA have been shown to be more susceptible to developing infections compared to non-RA patients, particularly of the skin and soft tissue. 1 Studies suggest that patients with RA are predisposed to developing infections due to primary defects in the cellular immune response. 2,3 Additionally, this predisposition to developing infections may be exacerbated by the immunosuppressive regimens often utilized as first-line treatment in RA, including methotrexate and biologics such as anti-tumor necrosis factor (TNF) inhibitors. Abatacept is a relatively newer agent developed for treating RA with inadequate response to TNF-α inhibitors. The medication selectively modulates the costimulatory signal required for T-cell activation. 4,5 It has been suggested that patients may have an increased risk of fungal infection with use of abatacept, including histoplasmosis, blastomycosis, aspergillosis, and systemic candidiasis. 6 -8 Although in the general population Aspergillus species account for a large proportion of invasive fungal infections of the skin, paranasal sinuses, and lungs, invasive infections by non-Aspergillus species including Fusarium and Curvularia species have been reported. 9
In the present case, we report an atypical, angioinvasive, and fungal infection of the auricle in the setting of RA treated with abatacept. Our patient responded well to surgical debridement and antifungal therapy and made a full recovery without evidence of recurrent or persistent disease. When considering autoimmune and vasculitic etiologies for necrotic, cutaneous lesions, clinicians should maintain a high level of suspicion for opportunistic infections, especially in the setting of an immunosuppressed patient. For cutaneous, necrotic lesions with evidence of invasive fungal species in these patients, we recommend early surgical debridement and empiric pharmacologic coverage of opportunistic infections.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.