
Abstract
Localization of parathyroid adenomas for treatment of primary hyperparathyroidism can be challenging. This retrospective study compared single-photon emission computed tomography/computed tomography (SPECT/CT), 4D-CT, and US studies in detection of adenomas prior to surgery. A retrospective chart review was performed on all consecutive patients with parathyroid adenoma presenting to an urban tertiary care medical center. A total of 58 patients (45 female, 13 male) underwent surgery for parathyroid adenoma. Patients aged 28 to 80 years (mean: 58.8) with parathyroid hormone levels ranging from 42 to 424 pg/mL (mean: 168). All patients underwent preoperative SPECT/CT with 20 mCi technetium-99m MIBI (99mTc-MIBI). Fifty-three patients had additional US imaging and 14 patients had 4D-CT scans. Additionally, 34 patients had injection of 20 mCi 99mTc-MIBI on the day of surgery. Pathological correlation was performed. Comparing SPECT/CT versus 4D-CT resulted in sensitivity (77% vs 80%), specificity (71% vs 75%), and accuracy (77% vs 79%). Ultrasound was less sensitive with similar specificity (44%, 86%, respectively). Combination of SPECT/CT and 4D-CT increased sensitivity to 88%, specificity to 100%, and accuracy to 89%. Combining SPECT/CT with US resulted in sensitivity of 85%, specificity of 83%, and accuracy of 85%. Intraoperative localization substantially improved in patients who received preoperative injections. The SPECT/CT remains the best imaging modality for preoperative localization of parathyroid adenomas with high sensitivity. Combining SPECT/CT with US resulted in increased sensitivity and accuracy. For suspicion of ectopic cases or suspicion of unidentifiable adenoma with negative scintigraphy, addition of 4D-CT is recommended. Intraoperative localization and adjunctive imaging may improve surgical management of patients with hyperparathyroidism.
Introduction
Primary hyperparathyroidism (PHPT) is a common endocrine disorder, with a prevalence of 1 to 7 per 1000. 1 Classically, PHPT is characterized by elevated parathyroid hormone (PTH) and hypercalcemia. Variations in phosphorus, alkaline phosphatase, and urinary calcium can be seen as well. Hypercalcemia, which if left untreated, can lead to long-term end-organ damage. An estimated 85% of cases of hypercalcemia can be attributed to PHPT, which warrants investigation into accurate diagnostic and treatment methodologies. 2 Although PHPT is most often sporadic it can be associated with familial syndromes such as multiple endocrine neoplasia (MEN 1 and MEN 2). 3
The most common form of PHPT is parathyroid adenoma, benign hyperplastic regions of parathyroid tissue that often produce excess PTH. A minority of PHPT is caused by multigland hyperplasia. 1 Rarely, tumors such as parathyroid carcinomas can also cause PHPT. 2 In contrast, secondary and tertiary hyperparathyroidism are generally reactionary responses to decreased calcium levels in the body or to kidney dysfunction, and generally cause multiple gland hyperplasia rather than a single adenoma. 4 The most definite treatment for PHPT is surgical, which is considered when patients develop symptoms or end-organ damage. 2 Standardized criteria for workup, management, and indications for surgical resection in hyperparathyroidism exist. 5 However, even after surgery is decided, adenoma localization can be difficult. In fact, up to 16% of adenomas can be ectopically located in the mediastinum. 6 Furthermore, it is not uncommon to encounter 2 concurrent adenomas, otherwise known as “double adenoma”. 7
Many imaging modalities have been utilized through the history of parathyroid adenoma surgery. The least invasive technique is a neck ultrasound (US). 8 The successful identification of a parathyroid adenoma with ultrasound is dependent on multiple factors, such as the technician’s proficiency, neck girth, lesion size, and confounding thyroid disease. Still, US is a useful modality, given its noninvasive and affordable nature. 8 -10
Historically, parathyroid scintigraphy has been the primary imaging modality of choice. Multiple radiopharmaceutical agents have been used over the past few decades, and currently technetium-99m MIBI (99mTc-MIBI) is the agent of choice. 11 The technique is based on the differential washout of the tracer from thyroid tissue compared to parathyroid tissue. 12 Single-photon emission computed tomography (SPECT) in combination with low-dose conventional computed tomography (CT) further assists in localization. 99mTc-MIBI SPECT/CT scans have increased the sensitivity and specificity of scintigraphy alone, most importantly assisting with anatomic localization. 13 -16 However, this method has difficulty localizing adenomas when thyroid nodules are present, when parathyroid adenomas are small, or if there is multigland disease. 17
Traditional CT initially is not popular given the difficulty distinguishing parathyroid adenomas from lymph nodes. Recently, protocol changes have resulted in a “4D-CT,” in which a late contrast washout phase is added. The utility of this modality arises from the washout time of the contrast agent in lymph nodes compared to parathyroid glands. 18 -21 However, on average, SPECT/CT is a lower radiation dose (7 mSv) compared to 4D-CT (10.8 mSv). 22,23 Other groups have attempted to use MRI with limited success. 24,25 Both of these modalities have increased cost, limited studies, and a lack of universally accepted protocols.
Of late, PET/CT has gained popularity. Multiple tracers have been trialed with variable results: 11C-L-methionine, 18-F choline, and 18F-fluorocholine. 26 -28 The literature on PET/CT in parathyroid imaging is very heterogeneous and needs larger trials to further elucidate the value. 29
In addition to preoperative localization, there are many immediate preoperative and perioperative techniques that assist with localization as well. For one, many surgeons use preoperative injections of 99mTc-MIBI with an intraoperative probe to localize the adenoma. 30 In fact, this method has been shown to help detect adenomas that were not visualized preoperatively on the MIBI scans. 31 Furthermore, most surgeons draw preoperative and postexcisional PTH levels to confirm excision of the adenoma. This is a very reliable and fast technique, as PTH is rapidly metabolized. 32 If the levels do not drop to a normal range within 15 to 20 minutes, the surgeon generally considers exploring for a second adenoma. 32 These techniques are most useful when the adenoma is difficult to localize preoperatively, when it is not in the suspected location, or if there is a second adenoma.
This retrospective study compares the efficacy of SPECT/CT versus US versus 4D-CT in the localization of parathyroid adenomas as well as the benefits of intraoperative localization. The goal of the study was to determine the utility and accuracy of the various imaging modalities, especially when used in combination.
Patients and Methods
This retrospective study evaluated all consecutive patients who underwent parathyroidectomy over a 3.5-year period (January 2015 through July 2018) at our institution. All patients with evidence of hyperparathyroidism who underwent surgery were reviewed. Patients with prior surgery for hyperparathyroidism were excluded. This study was approved by the institutional review board at our institution. No consent forms were required.
Fifty-eight patients (45 female, 13 males; mean age 58.8 years, range 28-80) who underwent parathyroid surgery were reviewed. Patients with PHPT had PTH levels ranging 42 to 424 pg/mL (mean: 168, median: 139) and preoperative calcium levels ranging 9.1 to 13.3 (mean: 10.7). All patients had immediate postoperative PTH levels and 27 patients had additional 6-month postoperative PTH and calcium levels assessed. All patients (58) underwent SPECT/CT imaging of the parathyroid within 6 months prior to surgery, 53 patients had additional US imaging, and 14 patients underwent 4D-CT scans (Table 1).
Demographics.
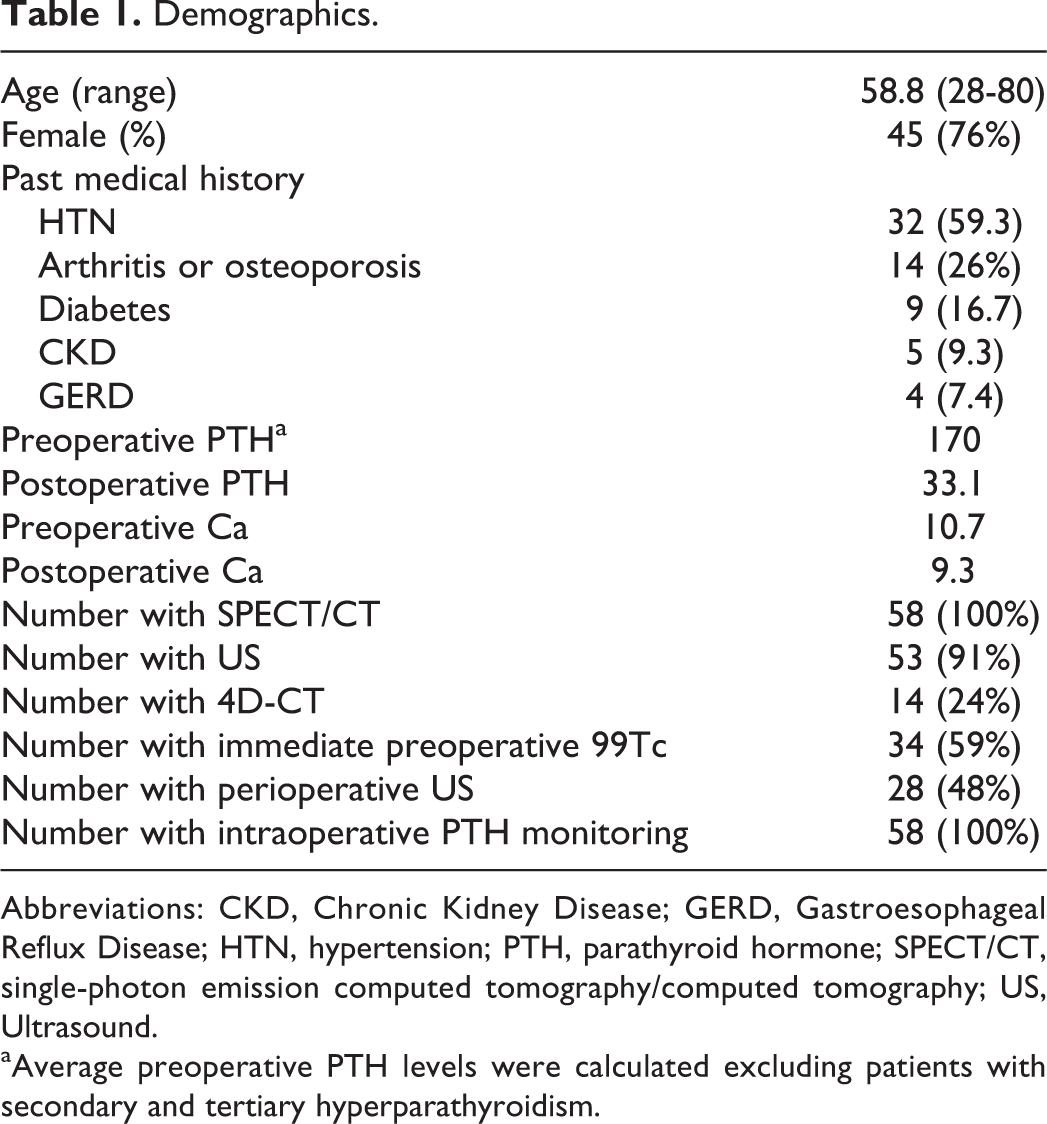
Abbreviations: CKD, Chronic Kidney Disease; GERD, Gastroesophageal Reflux Disease; HTN, hypertension; PTH, parathyroid hormone; SPECT/CT, single-photon emission computed tomography/computed tomography; US, Ultrasound.
aAverage preoperative PTH levels were calculated excluding patients with secondary and tertiary hyperparathyroidism.
The order of SPECT/CT and US varied for each patient. Ultrasound is routinely ordered in our practice for most head and neck patients undergoing parathyroid surgery to screen for possible thyroid nodules to determine need for concurrent thyroid surgery. It is common to order both examinations at the same visit. Of the 53 patients who underwent ultrasonography, 32 had US prior to SPECT/CT, and 21 had US performed after SPECT/CT. SPECT/CT studies were interpreted blindly to other imaging modalities. 4D-CT was ordered when other modalities were not clear or inconclusive due to small adenoma size or uncommon ectopic adenoma location.
99mTc-MIBI SPECT/CT
Single-photon emission computed tomography/CT of the neck and chest was performed on the Infernia SPECT (GE, Boston, Massachusetts) using a dual phase 99mTc-MIBI high-resolution protocol and 2 slice CT. Early acquisition was performed at 20 minutes after intravenous injection of 20 mCi 99mTc-MIBI. Subsequently, the early SPECT/CT was performed in 360° and reconstructed. Delayed imaging was performed at 2 hours. The energy window for 99mTc-MIBI was 140 keV ± 20% window.
Additionally, patients had preoperative injection of 10 to 20 mCi 99mTc-MIBI followed by single imaging at 20 minutes post injection for intraoperative monitoring. Preincisional background γ uptake was measured at the level of the thyroid isthmus, and ex vivo uptake of the adenoma was also obtained with a Neoprobe GDS machine (Devicor Medical Products, Inc, Cincinnati, Ohio).
Ultrasound
Ultrasound examination for parathyroid gland included a routine examination of the neck soft tissue with a TU 22 (Philips, Amsterdam, the Netherlands) using a 12-MHz linear probe to study for location, size, and vascularity. The patient was placed supine for the procedure, and all parts of the anterior and lateral cervical area, the upper mediastinum, and supraclavicular region were evaluated in at least 2 orthogonal views.
4D-CT
Four-dimensional CT was performed on a 64-detector iCT scanner (Philips, Amsterdam, the Netherlands). The protocol consisted of 3 imaging phases: #1 was a nonenhanced CT study; phase #2 and 3 consisted of contrast-enhanced phases from the angle of the mandible to the carina after intravenous administration of 75 mL of Omnipaque 350 followed by a 25-mL saline chaser. Arterial phase (#2) is captured 25 seconds after the start of the injection and the delayed venous phase (#3) at 80 seconds from the start of the injection. Images in 1-mm thick and 2.5-mm thick contiguous images for all 3 phases in the axial, coronal, and sagittal planes were used for interpretation.
Statistical Analysis
Statistical analysis was performed using JMP Pro 14.0.0 (SAS, Cary, North Carolina). Descriptive statistics was applied to all variables to estimate basic parameters such as mean, median, standard deviation, and range. Variables were compared using Pearson correlation, t test, χ2, and McNemar testing. Correlation between imaging results and postoperative pathology was performed to determine sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for detecting parathyroid adenoma for each modality. Cases of double adenoma were considered to be 2 separate results for analysis, resulting in 64 separate lesions.
Combined sensitivity and specificity were determined for a SPECT/CT and US group and a SPECT/CT and 4D-CT groups. Analysis was performed on a per lesion basis. A reading was considered to be a true positive if preoperative interpretation matched the operative findings (ie, right superior parathyroid), whereas a false positive was considered when imaging findings did not agree with intraoperative findings (ie, SPECT/CT reports right superior adenoma, intraoperative finding left inferior adenoma). A negative imaging finding in the presence of multigland hyperplasia was considered to be a true negative. Finally, in cases of a double adenoma, each adenoma was considered separately. For example, if imaging demonstrated a right superior adenoma and surgery found right and left superior, this was reported as a false negative and true positive.
Results
Fifty-eight patients were identified with previously untreated PHPT who had preoperative SPECT/CT and subsequent surgery. Four (6.8%) patients had secondary or tertiary hyperparathyroidism. Of those with PHPT, 42 (72%) patients had parathyroid single adenoma, 6 (10%) patients had double adenomas, and 5 (6.8%) patients had multigland hyperplasia. One (1.7%) patient was diagnosed with parathyroid carcinoma. Five (8.6%) adenomas were found to be ectopic, 2 (3.4%) of which were found in the superior mediastinum.
Average preoperative PTH level was 167 pg/mL (range: 42-424) and calcium level was 10.7 (range: 9.1-13.3). Postoperative PTH levels significantly decreased immediately to 9.3 pg/mL (P < .001). PTH levels 6 months postsurgery were also significantly decreased compared to preoperative levels: 64 pg/mL (P < .001). Postoperative calcium levels also significantly dropped 9.3 (P < .001). The average size of the adenoma was 1.02 grams (range: 0.1-4.0 g), and the largest average dimension was 1.79 cm (range: 0.4-3.5 cm).
On average, the missed adenomas (false negative) on SPECT/CT were significantly smaller than the detected adenomas (0.42 g vs 1.2 g; P < .0001). Additionally, the preoperative Ca levels correlated with the size (Pearson correlation: 0.419; P = .0018) and weight (correlation: 0.572; P < .001) of the adenoma (Figure 1). However, preoperative PTH levels did not correlate with the size (correlation: 0.132; P = .39) or weight (correlation: 0.132; P = .336). Examples of patients with their respective images are shown in Figures 2 –4.
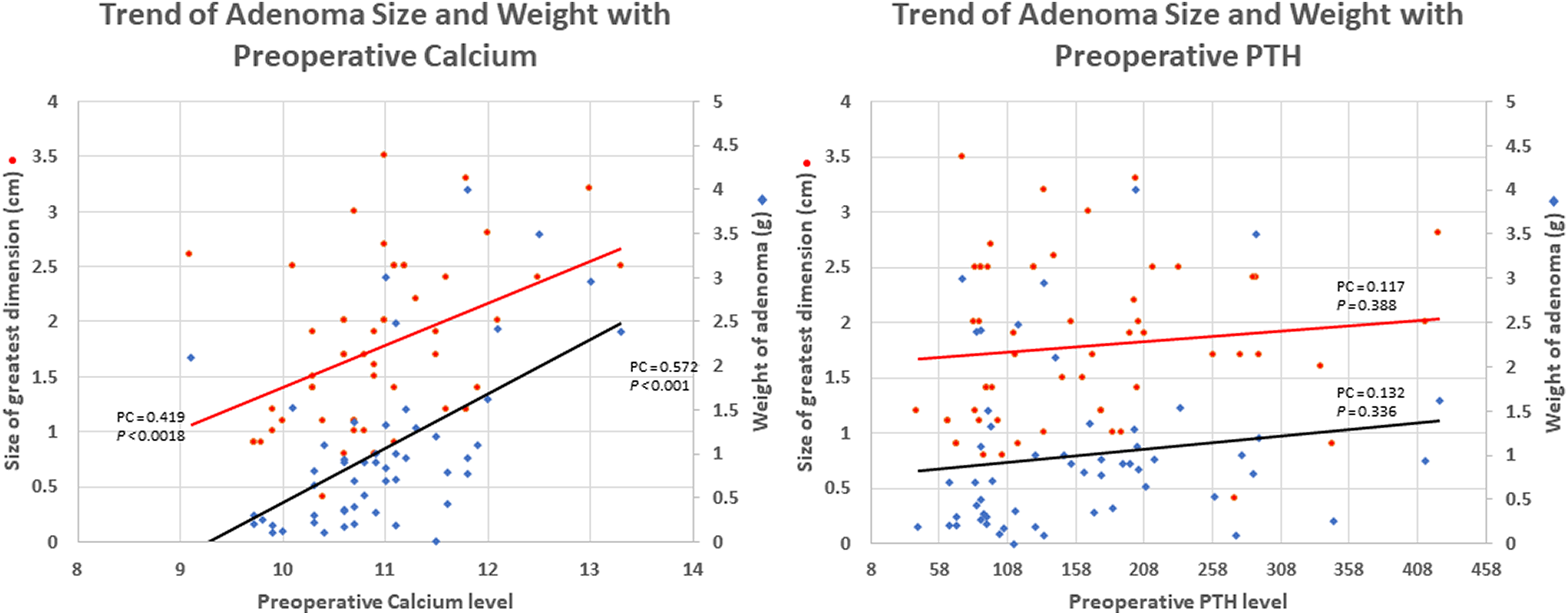
Preoperative calcium (left) was significantly associated with the weight and size while preoperative PTH was not. P values and correlation shown in this figure. PC indicates Pearson correlation; PTH, parathyroid hormone.
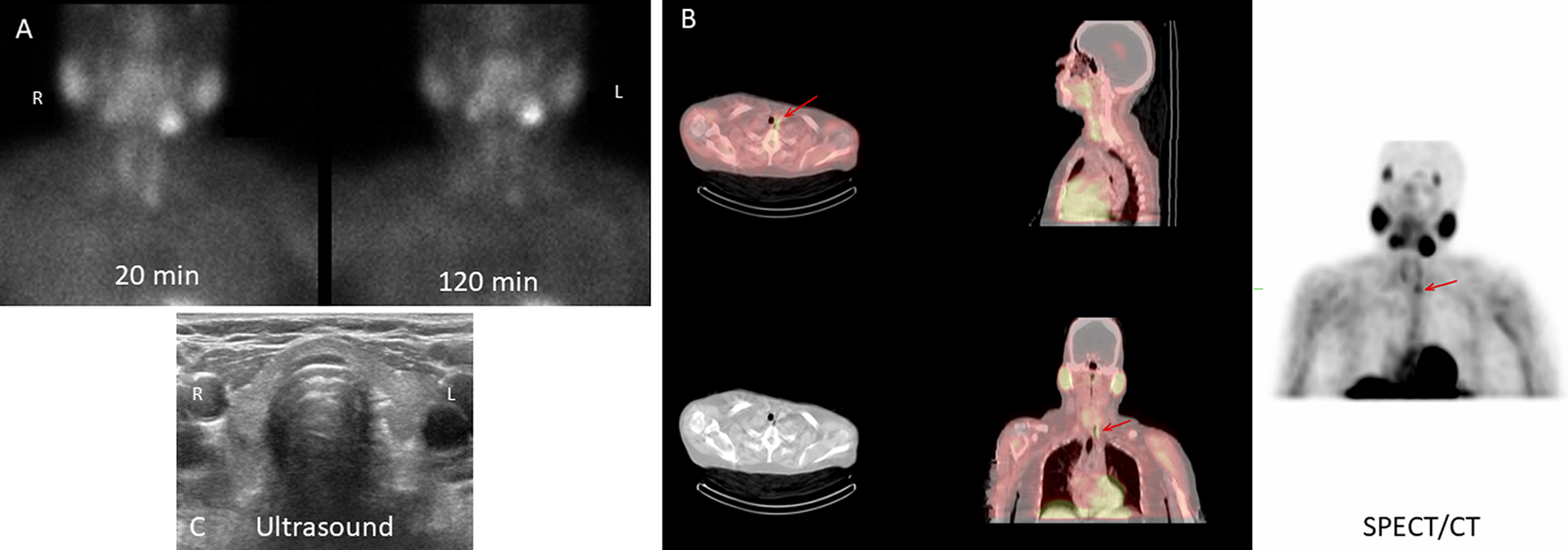
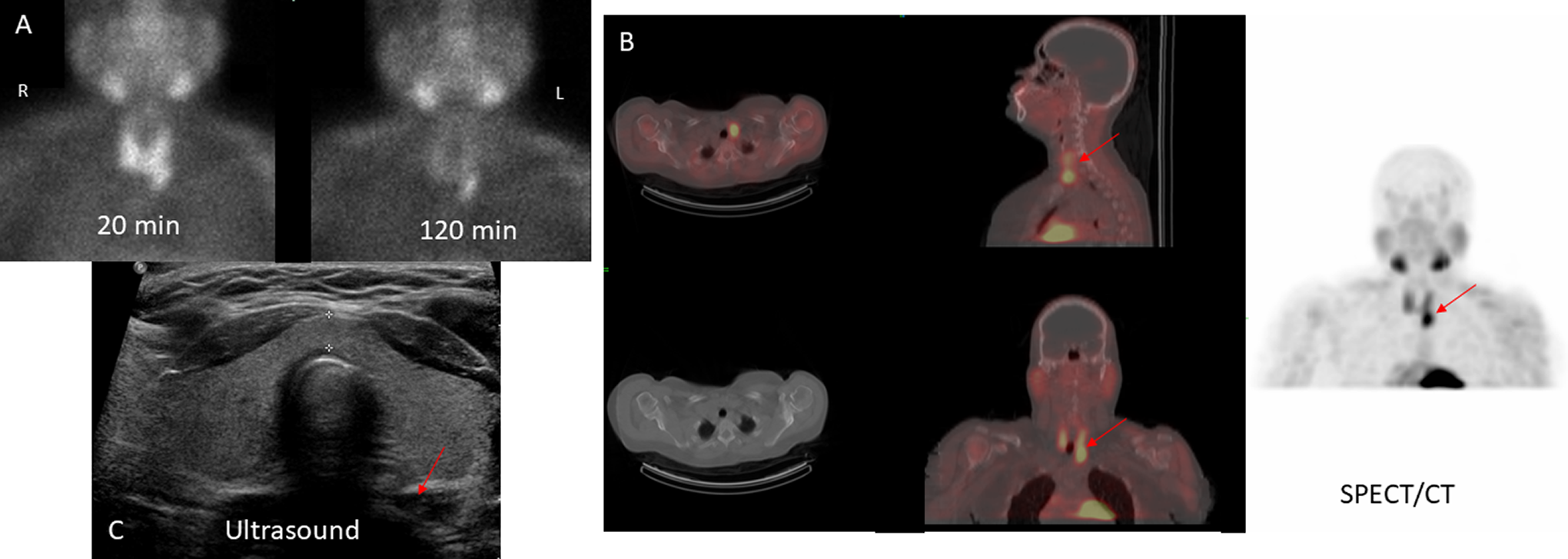
Seventy-year-old female with Ca 10.6 and PTH 171 had SPECT (A, B) demonstrating left inferior adenoma, and nondiagnostic US (C). Adenoma was successfully resected. PTH indicates parathyroid hormone; SPECT, single-photon emission computed tomography.
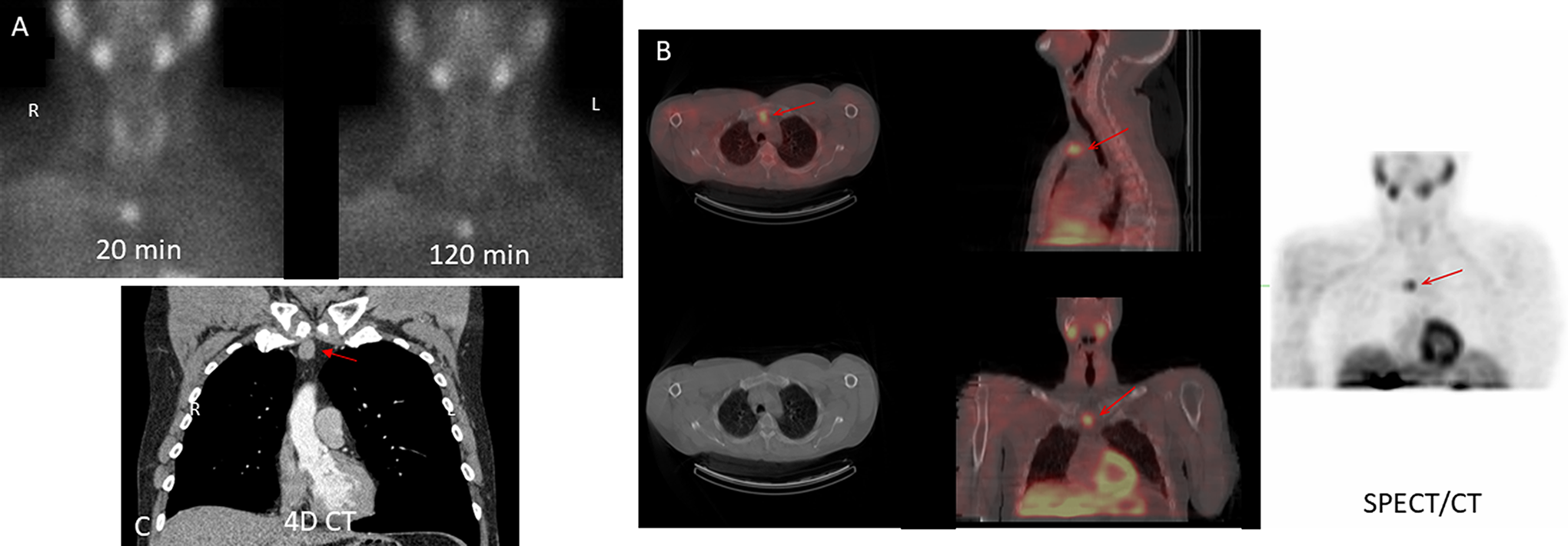
Fifty-three-year-old male with Ca 13.3 and PTH 85 had SPECT/CT (A, B) and 4D-CT (C) demonstrating an anterior mediastinal ectopic parathyroid gland that was successfully resected. PTH indicates parathyroid hormone; SPECT, single-photon emission computed tomography.
Fifty-four-year-old female with Ca 13.0 and PTH 135 had SPECT/CT (A, B) and US (C) demonstrating a left inferior adenoma that was successfully resected. PTH indicates parathyroid hormone; SPECT, single-photon emission computed tomography.
Results of SPECT/CT, US, and 4D-CT
Of the 64 suspected adenomas scanned, overall sensitivity of 99mTc-MIBI SPECT/CT, US, and 4D-CT with respect to intraoperative findings were 77%, 44%, and 80%, respectively, while the overall specificity was 71%, 86%, and 75%, respectively (Table 2). Accuracy was similarly distributed as well.
Overall Sensitivity, Specificity, and Accuracy, Per Lesion-Based Analysis.a
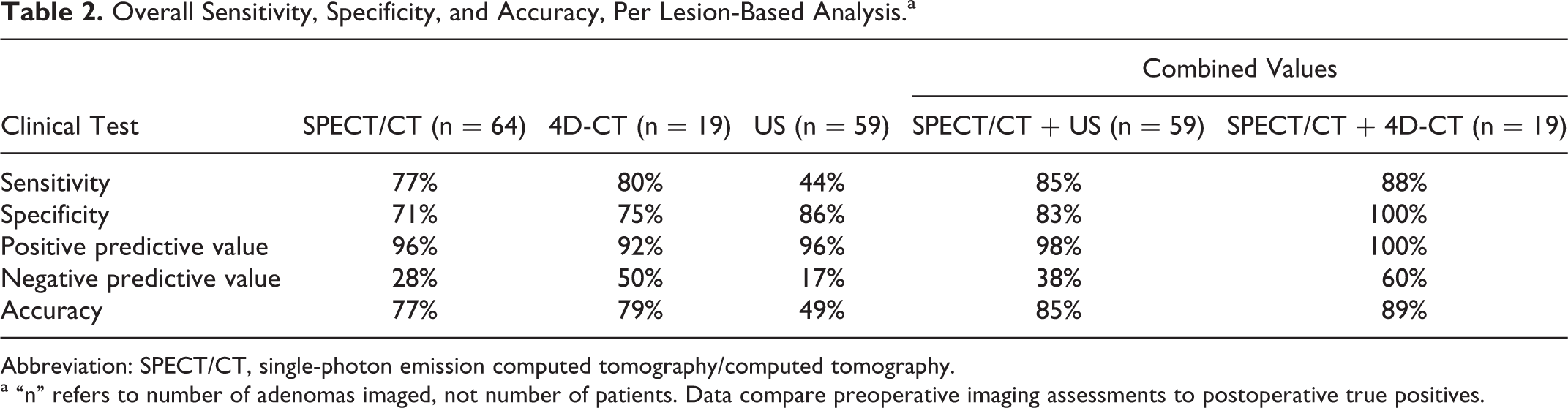
Abbreviation: SPECT/CT, single-photon emission computed tomography/computed tomography.
a “n” refers to number of adenomas imaged, not number of patients. Data compare preoperative imaging assessments to postoperative true positives.
Paired sensitivity and specificity were determined as well (Table 3) to compare various imaging modalities. SPECT/CT was significantly more sensitive and accurate compared to ultrasound alone (P = .003 and .009, respectively). Sensitivity and specificity of SPECT/CT and 4D-CT were not significantly different (P = .68, 1.0, respectively).
Paired Sensitivity, Specificity, and Accuracy, Per Lesion-Based Analysis.a
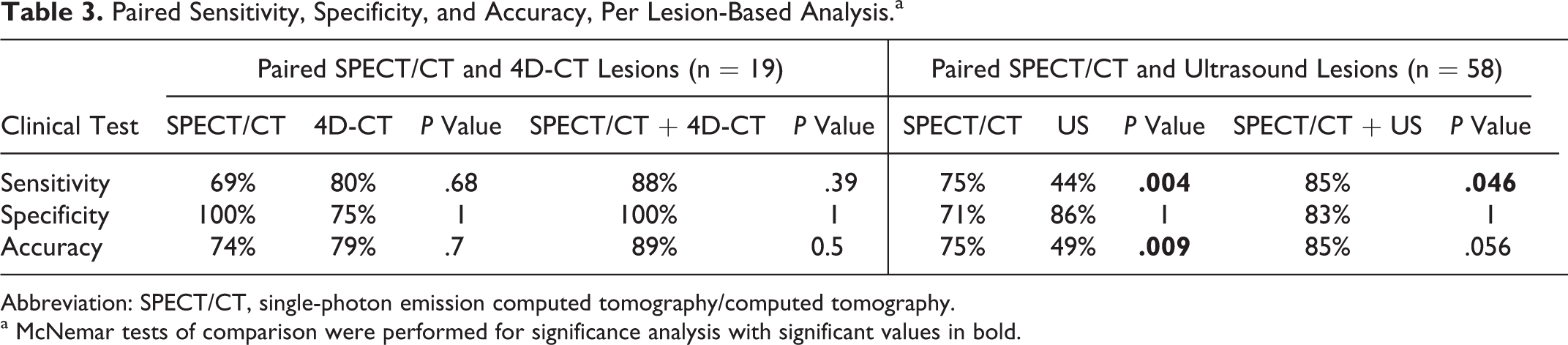
Abbreviation: SPECT/CT, single-photon emission computed tomography/computed tomography.
a McNemar tests of comparison were performed for significance analysis with significant values in bold.
Concordance and Combined Testing
The addition of ultrasound to 99mTc-MIBI with SPECT/CT increased the sensitivity, specificity, and accuracy compared to both modalities alone (Tables 2 and 3). Single-photon emission computed tomography/CT with addition of ultrasound was more sensitive compared to SPECT/CT alone (P = .046); however, there was no difference in specificity or accuracy. By itself, US was not very sensitive and had poor accuracy. The addition of US converted 5 false negatives on SPECT/CT to true positives, but failed to convert 8 false-negatives on SPECT/CT. Only 1 false positive was seen on US.
The addition of 4D-CT to SPECT/CT was more useful than US alone. The sensitivity, specificity, and accuracy of 4D-CT with SPECT/CT was not significantly different compared to SPECT/CT alone (Table 3, P = 0.68, 1.0, 0.7, respectively). Specifically, there were 5 false negatives on SPECT, 3 of which were identified on 4D-CT and converted to true positives. The 2 false negatives on combined testing were cases of double adenomas. In one case, the larger (0.96 g) left superior adenoma was correctly identified by both modalities, but the smaller (0.77 g) left inferior was gland was missed. In the other case, SPECT/CT correctly identified a left inferior adenoma but missed the intrathymic adenoma. 4D-CT missed both of these adenomas and incorrectly noted a possible ectopic gland in the left neck, found to be negative (recorded as false positive). In this case, the clinical decision to obtain 4D-CT was due to an unexpected midline uptake on SPECT/CT. While this was correctly identified on 4D-CT as thymus, theintrathymic parathyroid adenoma was not identified.
4D-CT had 3 false negatives, 2 of which were double adenoma cases as previously described. In the third case, the region was correctly identified on SPECT/CT; 4D-CT was ordered additionally due to low uptake on SPECT/CT and for better anatomic mapping, but failed to identify the adenoma (right superior, 0.89 g). On the other hand, 4D-CT converted 3 false-negative cases on SPECT/CT to true positives. These 3 cases had suspicious ultrasound findings, so 4D-CT was ordered additionally.
Ectopic Glands
A total of 5 ectopic parathyroid glands were encountered in this study. One substernal mass was only correctly identified on 4D-CT and SPECT/CT. Two intrathymic adenomas were encountered, one of which was identified by all modalities, and the second was identified only intraoperatively. 4D-CT accurately identified retroesophageal and thyroesophageal groove adenomas. Of the 3 adenomas in these locations, 1 was missed on SPECT/CT but identified on 4D-CT.
Double Adenomas
There were 6 cases of double parathyroid adenoma. On average, cases with double adenomas had significantly lower preoperative PTH compared to cases with single adenomas (PTH 101 vs 180; P = .019). Preoperative Ca levels were not significantly different (P = .29). In addition, on average, double adenoma glands were smaller compared to single adenomas when double adenomas were weighed individually (0.42 g vs 1.20 g; P = .0047). However, the combined double adenoma weight was not significantly different from single adenoma weights (0.79 vs 1.2 g; P = .13). Five of these cases had at least 1 gland correctly identified on preoperative imaging.
Intraoperative Testing
Twenty-eight patients had intraoperative US performed prior to beginning the surgery. All patients had intraoperative PTH levels checked to confirm excision of adenoma. All but one single adenoma case had adequate drop in PTH level down to a normal after excision. In this case, a multigland exploration was performed to search for a second adenoma that was not identified. All double adenoma cases had adequate drop in PTH level down to normal after excision of both masses. In addition, 34 patients had preoperative 99mTc injection in the morning prior to surgery. All of these patients had ex vivo γ uptake of the adenomas confirmed intraoperatively prior to completion of surgery to verify that parathyroid adenoma was identified.
Discussion
Parathyroid adenoma surgery can be challenging without adequate preoperative planning. Although the traditional 4-gland exploration for parathyroid adenoma is quite successful, more often a focused parathyroidectomy is performed, facilitated by intraoperative technologies and preoperative imaging. Some authors support this methodology due to less surgical time, smaller incision, shorter duration of stay, less postoperative pain, and lower rates of postoperative hypocalcemia. 33 Proper application of focused parathyroidectomy hinges on adequate preoperative localization of the parathyroid adenoma. As such, a variety of imaging modalities are available; however, there is no universally accepted algorithm for imaging.
Although traditionally US and 99mTc sestamibi have been popular methods, sensitivity and specificity are varied. Recently, various imaging modalities such as 4D-CT, PET, and MRI have been used with mixed success. At our institution, the standard workup for all patients with suspicion for PHPT is 99mTc MIBI SPECT/CT imaging. Most patients also have head and neck US as well. 4D-CT is traditionally reserved for patients with unclear SPECT/CT results with a continued suspicion for adenoma.
SPECT/CT generally missed smaller adenomas, which is consistent with established literature. 34 In this cohort, preoperative Ca was predictive of the size and weight of the adenoma. Thus, for patients with hyperparathyroidism with low calcium levels, SPECT/CT seems to be inadequate to reliably detect adenoma location. Some groups suggest a scan and lab-directed approach, with focused parathyroidectomy in patients with higher calcium and PTH levels, and multigland exploration for those with lower lab levels and nonlocalizing MIBI. 35
However, many groups suggest the addition of more imaging such as US to scintigraphy, which can be advantageous to improve accuracy and sensitivity. 8,36,37 Similarly, in our cohort, we demonstrated a similar improvement in detection. Primarily, the addition of US converted 5 of 12 false negatives to true positives. Additionally, US is helpful in providing anatomic mapping of the thyroid gland, allows for planning for concurrent thyroidectomy or hemithyroidectomy if necessary, and is low cost. It is important to note that US alone is not adequate as a single modality to image the parathyroid glands due to low sensitivity and accuracy. Although not accurate by itself, US is a useful adjuvant to SPECT/CT due to the improved sensitivity and the additional thyroid mapping benefits.
With respect to 4D-CT, the overall accuracy was not significantly different compared to SPECT/CT. Even though 4D-CT did convert 3 false negatives to true positives on combined analysis, this was not sufficient to raise the sensitivity, specificity, or accuracy enough to be statistically significantly different (Table 3). As detailed above, 4D-CT was particularly useful in identifying ectopic glands such as those in the mediastinum, thymus, thyroesophageal groove, and retroesophageal space but was not helpful in identifying double adenomas. This is consistent with established literature, as 4D-CT is known to miss smaller lesions and cases with multiple adenomas. 38 The main utility of 4D-CT in this review was in cases of negative or nonlocalizing SPECT/CT scans.
From this cohort, it is difficult to justify the routine use of both SPECT/CT and 4D-CT in all patients with suspected parathyroid adenoma. Overall, SPECT/CT has good sensitivity and specificity and may be considered as the first-line imaging modality. Although 4D-CT had comparable sensitivity and specificity, there were fewer cases with this methodology and further studies would be necessary to determine whether 4D-CT should replace SPECT/CT in our institution. Additionally, SPECT/CT with 4D-CT was not statistically significantly different from SPECT/CT with US, or SPECT/CT alone. The overall radiation exposure with 2 modalities requiring CT makes it hard to justify 4D-CT with SPECT/CT as a reasonable combination for every patient. Although Table 2 demonstrates high sensitivity and specificity for SPECT/CT + 4D-CT, our study has a low number of 4D-CT scans which may contribute to the lack of statistical significance. Thus, we recommend reserving this 4D-CT for certain situations such as cases with ectopic glands, especially in patients suspected to have adenoma but have unidentified lesions on initial imaging. Rather, SPECT/CT with the addition of ultrasound is more sensitive than either modality alone and should be routinely recommended.
Single-photon emission computed tomography/CT is known to miss smaller adenomas. Since preoperative calcium levels can be predictive of adenoma size, one can consider using an alternative modality to SPECT/CT in these cases. However, 4D-CT has been shown to miss smaller adenomas as well and may not be the best alternative, though smaller adenomas were not missed in our study. 38 No patient had MRI or PET/CT, as these modalities were not routine for parathyroid disease at our institution. Future studies with MRI and PET/CT may demonstrate more benefit.
We believe the main limitation of this study is the small sample size, especially for the subgroups with 4D-CT. More patients with each imaging modality would allow for better comparisons between the subgroups. We do not believe there was any bias in our patient selection criteria, as the patients were consecutively selected out of surgical cohorts. However, the retrospective nature of this study is limited by the tiered imaging process, without blinded interpretations. This may introduce some confirmation bias and result in less disagreement among imaging modalities.
Conclusion
This retrospective study compares the sensitivity, specificity, and accuracy of SPECT/CT, US, and 4D-CT alone and combined, as well as benefits of additional γ probe localization. Compared to ultrasound, SPECT/CT is more a sensitive and accurate to preoperatively identify parathyroid adenomas. The addition of US makes the specificity more significant; however, US cannot be used as a single modality due to low sensitivity and accuracy. SPECT/CT is less sensitive in cases with double adenomas or small adenomas. SPECT/CT and 4D-CT do not vary significantly, but on a per lesion-based analysis, 4D-CT is beneficial for those cases with suspected ectopic glands, or cases with negative scintigraphy with high clinical suspicion for single adenoma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.