
Abstract
Otology ENT Clinic Case
The patient is a 19-year-old man with congenital bilateral sensorineural deafness who underwent right-sided cochlear implantation in 2002, at the age of 3. Approximately 16 years postsurgery, in 2018, the patient started to complain of increasing pain, tenderness, and edema formation in the right retroauricular region, immediately above the implant. The edema was evenly distributed over the entire casing of the implant and the patient negated any recent trauma to the implant area. Due to symptom intensity, the patient was unable to continue regular use of the device. The device itself did not show any signs of malfunction. No signs of trauma or infection were noted and oral antibiotic (amoxicillin and clavulanic acid) treatment was administered for 7 days. The pain subsided, but the edema persisted, disabling implant use. A revision operation was planned to prevent further damage to the surrounding tissue and the implant. Preoperatively, an X-ray of the right temporal region showed a diastasis between the processor and the internal magnet of the implant measuring up to 20 mm (Figures 1 and 2). The first revision surgery was performed in May 2018. Intraoperatively, an abundance of fibrous subcutaneous tissue was found and excised, thinning the tissue overlying the implant. Residual hematoma was also found surrounding the internal magnet and was evacuated completely. Dexamethasone was applied into the surgical area. In the postoperative period, the patient received peroral antibiotic treatment (2 × 200 mg of cefpodoxime per day for 7 days). There were no complications in the immediate postoperative period. Six weeks following revision surgery, the patient was without any symptoms and had no trouble with using his implant. In July 2018, the patient again began to feel retroauricular pain, edema, and trouble using the implant due to recurring edema. A second revision operation was performed that same month. Intraoperatively, a substantial amount of fibrous tissue subcutaneously and hematoma surrounding the implant were again encountered. The subcutaneous tissue was re-excised and was sent for histopathological examination. The hematoma was evacuated and a swab sample was sent for microbiological analysis. The implant was completely exposed, and neo-ossification was noted in its posterior third, with bone overlying the posterior segment of the implant, as well as some unusual staining on the silicone implant (Figure 3). The bone was drilled away from the implant and the casing was fully mobilized. The implant magnet was replaced with a new one provided by the manufacturer’s support staff and the casing was covered with vancomycin powder. The patient was then treated with intravenous antibiotic treatment (ceftriaxone 2 × 1 g/d) for 4 days until discharge, when the treatment was changed oral antibiotics (cefpodoxime 2 × 200 mg/d for 7 days). The postoperative period was uneventful. The hematoma swab cultures remained sterile. The histopathological report of the fibrous tissue noted presence of diffuse pervasion of mono- and polymorphonuclear cells.
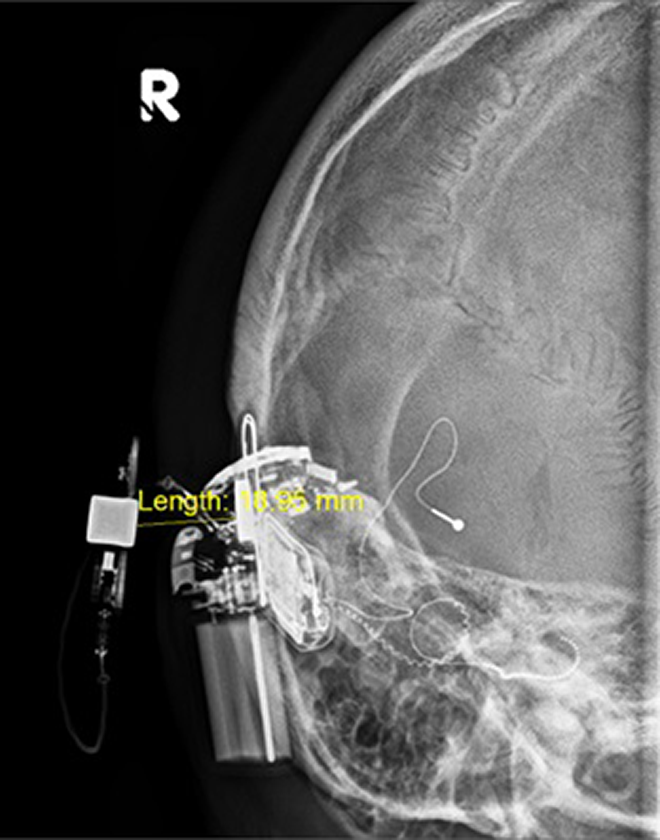
Preoperative X-ray image showing a diastasis of about 18 to 20 mm between the internal and external electrode.

Preoperative X-ray image showing a diastasis of about 18 to 20 mm between the internal and external electrode.
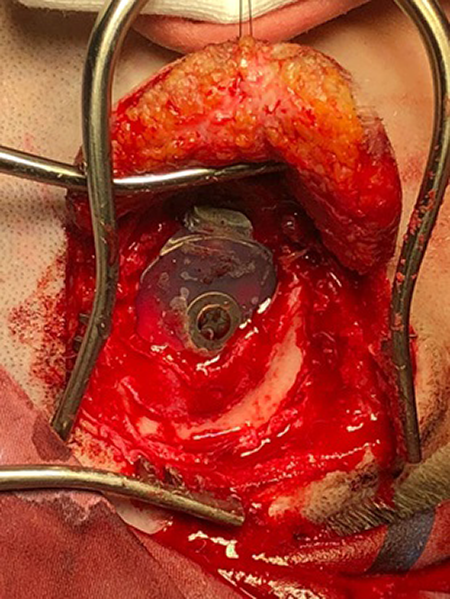
After exposing the implant, bone formation and unusual staining were noted on the silicone implant.
Discussion
Review articles focused on delayed complications of cochlear implantation found that only 48 (0.9%) of 5486 patients developed seromas or hematomas, the majority of which required only conservative therapy. 1,2 Delayed onset of pain and hematoma formation after cochlear implantation, which are complications encountered in this case report, are issues that are rarely encountered. 3 Current treatment strategies suggest conservative hematoma evacuation through needle aspiration and additional diagnostic procedures to account for underlying etiological factors such as infection, coagulopathies, or repeated head trauma. 3 -5 Pain has been reported as an isolated delayed-onset complication and regarded as a possible early symptom of cochlear implant malfunction. Some authors also suggest that delayed-onset pain should be considered a major complication since a significant amount of these patients require revision surgery. 2 Another recent report on 5 patients with delayed onset of pain in the region surrounding the implant showed that revision surgery and device explantation relieved the symptoms. Subsequent reimplantation was uneventful and no reason for initial pain onset could be identified. 6 There have been studies published mentioning neo-ossification that was found in revision surgery, but this was related to the ossification of the cochlea and the mastoid cavity. 7 One study found that intracochlear osseous tissue was more present in cases where the electrode was folded, though that was not the case in our patient. 8 In our case, there was no ossification of the cochlea, mastoid cavity, or the electrode, nor was bone dust used in prior surgeries in the region in which the neo-ossification occurred. No apparent cause for excessive fibrous tissue formation, hematoma formation, or neo-ossification was noted.
Footnotes
Authors’ Note
This case presentation was approved by the University Hospital Centre Sestre milosrdnice, Zagreb, Bioethical Board adhering to the Helsinki Declaration of 1983. Full written informed consent was obtained from the patient in using images of tissue samples and radiologic imaging after discussing the details of the case report contents. All of the authors have read and approved the manuscript, and all authorship contributions have been verified to adhere to ICMJE guidelines.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.