
Abstract

Introduction
Rheumatoid arthritis (RA) is a common disabling autoimmune disease characterized by inflammation of synovial joints including joints of the larynx. 1 Symptoms range from foreign body sensation and hoarseness to severe airway compromise. These symptoms are invariably due to impaired mobility of the vocal folds with potential narrowing of the glottal chink.
Based on a literature review on RA and vocal fold mobility, there are numerous reports on acute airway obstruction secondary to bilateral involvement of the cricoarytenoid joints, 2,3 with only one report on unilateral cricoarytenoid joint involvement. Kumai et al reported the case of a 57-year-old lady with 10-year history of RA who presented with sudden onset aphonia due to insufficient adduction of the left vocal fold that was successfully treated surgically by arytenoid adduction. 4
The authors of this manuscript report the second case of RA presenting with dysphonia due to unilateral cricoarytenoid joint involvement that was managed successfully by injection laryngoplasty as an office procedure.
Case Report
This is the case of a 53-year-old gentleman diagnosed with RA who presented with few months history of dysphonia associated with aspiration to fluid intake. Patient denied any shortness of breath or other airway symptoms. Perceptual evaluation revealed grade III dysphonia with marked breathiness. On laryngeal videostroboscopy, he had right unilateral vocal fold paralysis in the paramedian position with incomplete closure of the vocal folds during phonation (see Figure 1). A computerized tomography of the head and neck revealed increased bone density and narrowing of the left cricoarytenoid joint and ankylosis of the right cricoarytenoid joint (see Figure 2). Patient underwent injection laryngoplasty and a 0.5 mL of Restylane was injected in the right vocal fold lateral to the vocal process in order to achieve medialization (see Figure 3). Patient had marked improvement in voice quality following the procedure with an increase in the maximum phonation time from 4 to 10 seconds and a decrease in the rating of all perceptual parameters from G3R2B3A3S3 to G1R1B1A0S1.

Fiberoptic endoscopic view showing fixed right vocal fold in the paramedian position with bowing.
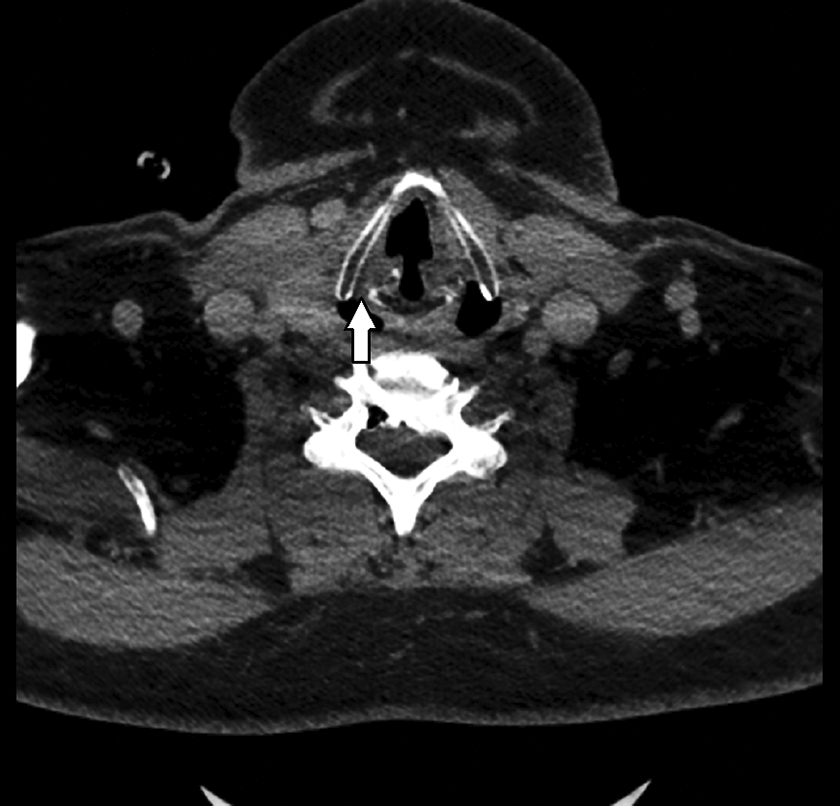
Computerized tomography showing increased bone density and narrowing of the left cricoarytenoid joint and ankylosis of the right cricoarytenoid joint (arrow).

Fiberoptic endoscopic view showing the right vocal fold bulging following the transoral injection laryngoplasty.
Discussion
Cricoarytenoid joint arthritis is diagnosed by a combination of laryngoscopy and computerized tomography of the larynx. In the acute phase, laryngoscopy usually reveals mucosal erythema and swelling in the region of the arytenoids. Computerized tomography is used to further assess soft tissue density, volume changes, fibrosis, and ankylosis at the level of the cricoarytenoid joint. As a diarthrodial joint with a synovial lining and a ligamentous capsule, the cricoarytenoid joint is subject to inflammatory changes that may start at the level of the synovial lining then progress to the articulating surface causing fibrosis and later ankylosis. 5 Other etiologies include the formation of rheumatoid nodules in the vocalis muscle or near the cricoarytenoid joint hindering its movement, 6 abductor muscle paralysis due to demyelination and degeneration of the ipsilateral recurrent laryngeal, 7 and last but not least cervicomedullary compression due to rheumatoid involvement of cervical spine. 8
In conclusion, patients with RA presenting with change in voice quality and history of aspiration should alert the physician for possible unilateral cricoarytenoid joint involvement. When impaired mobility of the vocal fold is present on laryngeal endoscopy, high-resolution computerized tomographic examination can assist the physician in diagnosing insidious cricoarytenoid joint involvement. In these cases, early intervention with injection laryngoplasty is recommended.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.