
Abstract

A 21-year-old man with a sensation of pressure over the right medial canthal area was referred to our hospital. The findings of ophthalmologic examinations performed at a private clinic were nonspecific. He had no orbital symptoms, such as visual disturbance, limited orbital movement, epiphora, and nasal symptoms. An endoscopic nasal examination revealed no specific findings. Paranasal sinus computed tomography (CT) was performed for evaluating his symptoms. The CT images revealed a homogenous and expansile mass that filled the right agger nasi cell located anterosuperior to the attachment of the right middle turbinate (Figure 1).
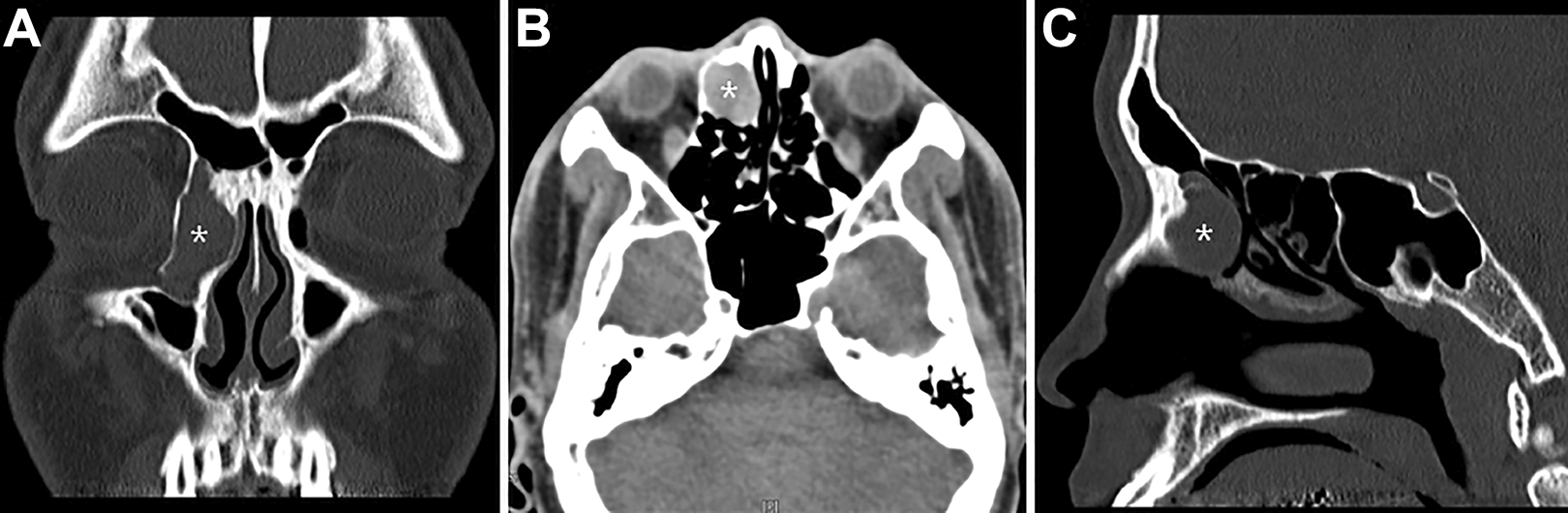
Coronal (A), axial (B), and sagittal computed tomography (CT; C) images of the nose and paranasal sinuses show a homogenous and expansile mass (asterisk) filling the agger nasi cell located anterosuperior to the attachment of the right middle turbinate.
On the basis of a suspicion of an isolated mucocele in the right agger nasi cell, we performed endoscopic sinus surgery under general anesthesia. When the lesion was punctured using a sickle knife to verify the mucocele cavity location, thick mucoid secretions were immediately released (Figure 2A). The cavity contained thick mucus and its contents were suctioned. The anterior wall of the mucocele was widely removed carefully by using a microdebrider and cutting forceps (Figure 2B). His postoperative course was uneventful, and the sensation of pressure over the right medial canthal area disappeared. The marsupialized cavity remained clear at the 5-month follow-up.
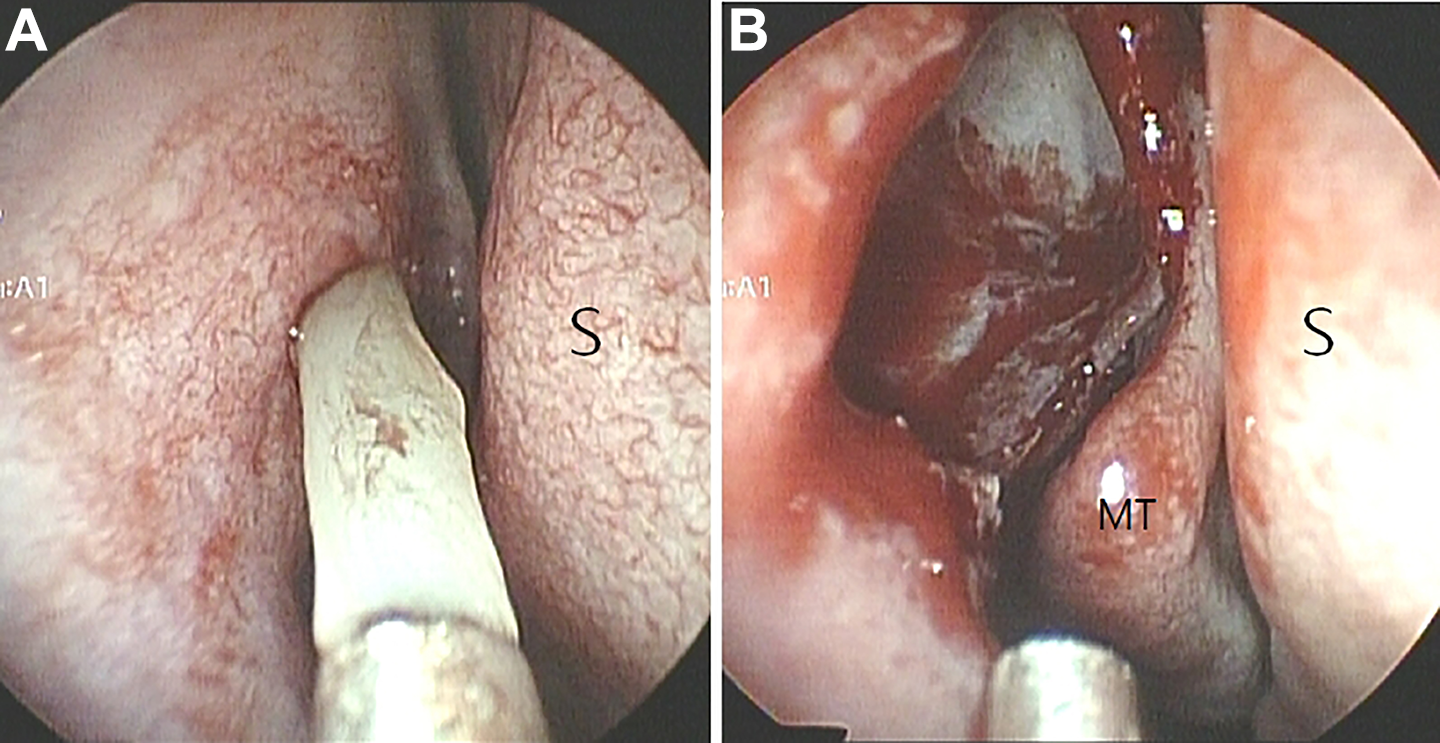
A, Endoscopy reveals the mucocele cavity containing thick mucus. B, Endoscopy shows the mucocele cavity after the wide removal of its anterior wall by carefully using a microdebrider and cutting forceps. MT indicates middle turbinate; S, nasal septum.
Paranasal sinus mucoceles (PSMs) are epithelium-lined cystic masses usually resulting from the obstruction of the sinus ostia due to trauma, inflammation, or tumors. The ethmoid and frontal sinuses are common sites of PSM development, while the maxillary and sphenoid sinuses are relatively uncommon locations. 1
The pneumatized agger nasi cell appears as an elevated region anterosuperior to the attachment of the middle turbinate. On endoscopic examination, the agger nasi cell can appear as an eminence anterior to the insertion of the middle turbinate. Any disease process affecting the lateral wall of the agger nasi cell can spread to the adjacent lacrimal sac and produce epiphora. The presence of a marked bulging anterosuperior to the attachment of the middle turbinate on endoscopy may indicate disease in this agger nasi cell. To the best of our knowledge, an isolated mucocele in an agger nasi cell has been rarely reported.
Computed tomography should be considered the diagnostic methods of choice. On CT without contrast enhancement, a soft-tissue mucocele mass with an expansile, homogenous appearance can be visualized. Therefore, a definitive diagnosis of the presence of mucocele in the agger nasi cells can be made by using CT.
The symptoms of PSM vary according to the location of the mucocele and could be classified as nasal and orbital symptoms. In case of frontoethmoidal mucoceles, orbital symptoms occur more frequently than do nasal symptoms. 2 Orbital symptoms, such as proptosis, frontal headaches, and limited orbital movement, are related to the compression caused by PSMs. 3 However, in case of isolated agger nasi cell mucocele, only a sensation of pressure or pain over the medial palpebral ligament may be present. Generally, simple drainage and marsupialization of the mucoceles have been performed with favorable long-term results. 4
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported by Wonkwang University in 2020.