
Abstract

Transesophageal echocardiography (TEE) is a safe and relatively noninvasive procedure, introduced in the operating room in the early 1980s during cardiac, major vascular, and transplantation surgery, as well as in emergency and intensive care medicine. 1 However, the insertion and manipulation of the ultrasound probe can cause pharyngeal, esophageal, or gastric trauma.
The aim of this article is not to describe a new clinical condition, but to show an unusual and sneaky case of hypopharyngeal TEE-related complication in which a nonsurgical treatment allowed for a good recovery without further sequelae.
An 87-year-old man was admitted to the emergency department complaining of progressive dysphagia and neck pain of 5-day duration. His medical history was positive for hypertension and atrial fibrillation, and 6 days before he was submitted to TEE. The physical examination revealed tenderness and crepitus on the left anterolateral area of the neck. The fiber-optic endoscopic evaluation showed a mild mucosal edema of the pyriform sinus (Figure 1A). Laboratory analysis revealed an elevation of the white blood cell count (16.61 × 103/μL). A computed tomography (CT) scan imaging showed a left parapharyngeal abscess with emphysema of the soft tissues of the neck (Figure 1B-D). The patient underwent ultrasound-guided needle aspiration of the abscess, and the purulent material was sent for culture. An empiric intravenous antibiotic treatment (piperacillin/tazobactam) was initiated. Clinical conditions progressively improved and the patient regained the ability to swallow within 5 days from admission. The culture was positive for Enterococcus faecalis, and the antibiogram confirmed the appropriateness of the antibiotic therapy, which was maintained for a total of 14 days. A CT scan confirmed the resolution of the abscess, and the patient was discharged after having completed the antibiotic therapy.
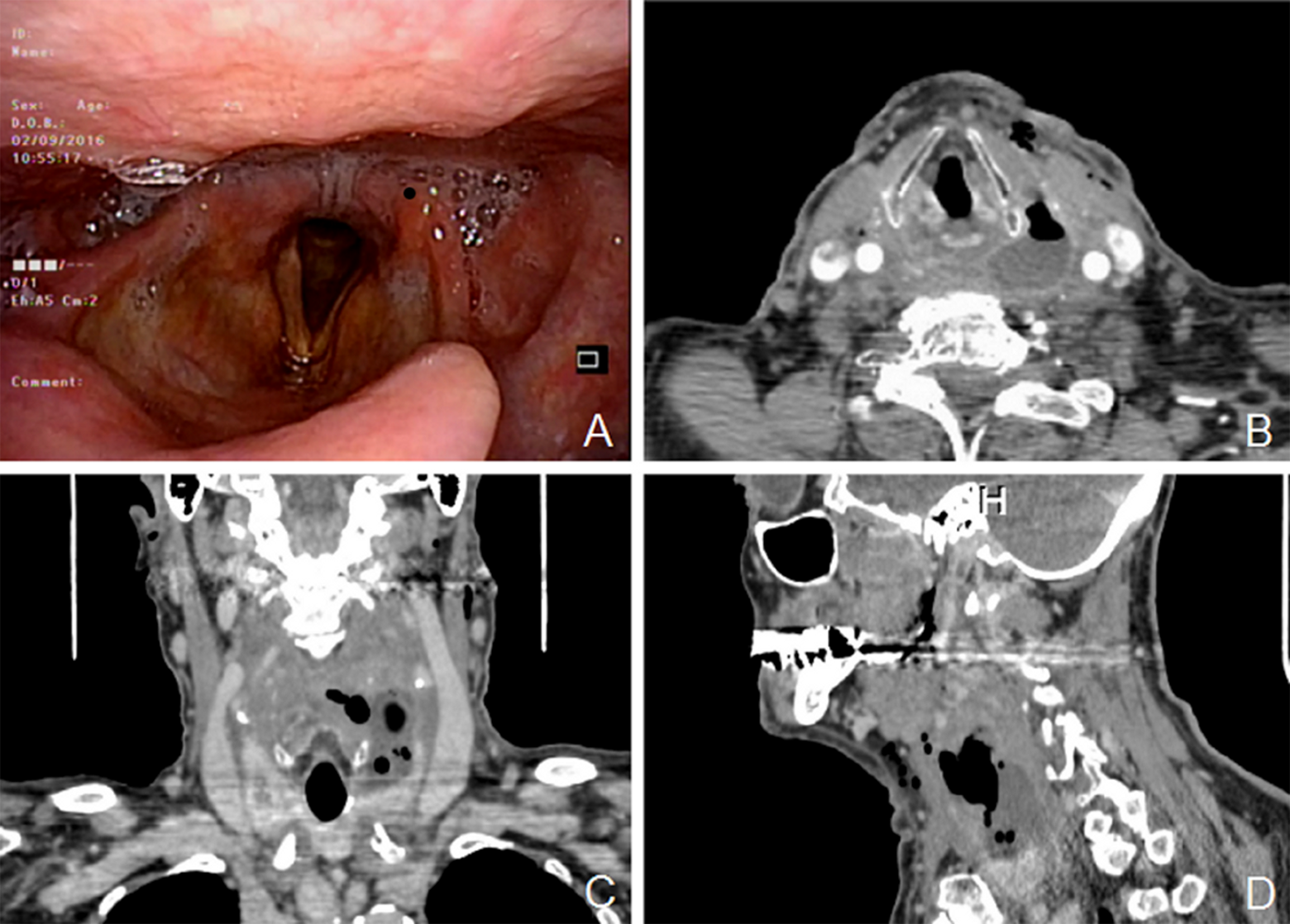
Fiber-optic nasendoscopy showing a swelling of the mucosa of the left pyriform sinus (A). Axial (B), coronal (C), and sagittal (D) computed tomography (CT) scan showing the left parapharyngeal abscess.
The incidence of major TEE-related complications range from 0.2% to 0.5% and mortality is reported to be <0.01%. 2 -5 Gastrointestinal perforation after TEE has been reported with an incidence between 0.01% and 0.04%, 6,7 and it is usually associated with severe morbidity, depending on mode of management and time to diagnosis. Mortality range from 10% to 56%. 8,9
The hypopharynx is the site of rupture in about 20% of cases. 8 During TEE probe insertion, one of the pyriform sinuses may be injured if the probe gets lodged in it.
Risk factors for perforation after TEE are gastroesophageal pathology (eg, Zenker’s diverticulum, esophageal stricture or obstructing mass, fibrosis secondary to prior chest radiation), distorted anatomy (eg, massive cardiomegaly, tracheoesophageal fistula, or atresia), and resistance to probe insertion. 10 Also, advanced patient age can increase the risk of perforation, as reported by Min et al. 3 Anyway, TEE does not represent a usual cause of deep neck infections, as demonstrated by a recent retrospective, single-institution study. 11
Patients complaining of neck pain, dysphagia, fever, or other suspicious symptoms after TEE should be promptly evaluated with a fiber-optic laryngoscopy and CT scan to rule out potential life-threatening complications such as hypopharyngeal perforation and/or deep neck infection. Conservative management, consisting in ultrasound-guided aspiration of the abscess and systemic intravenous antibiotic therapy, has proven to be effective.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.