
Abstract

A 61-year-old woman with a history of a progressively enhancing chronic left cheek mass presented to our institution for evaluation. Physical examination revealed a soft, nontender 8-cm nodule with distinctive bluish discoloration in the left parotid region. It demonstrated intermittent fluctuation in size and was fully compressible upon palpation. The patient endorsed regional warmth and skin redness in association with the mass. She denied pain, numbness, weakness, or pulsatile sensation. A computed tomography (CT) examination of the head and neck revealed a left parotid mass and associated regional lymphadenopathy. Magnetic resonance (MR) and angiogram of soft tissue mass of the neck was performed (Figure 1) revealing findings consistent with a venous malformation (VM).
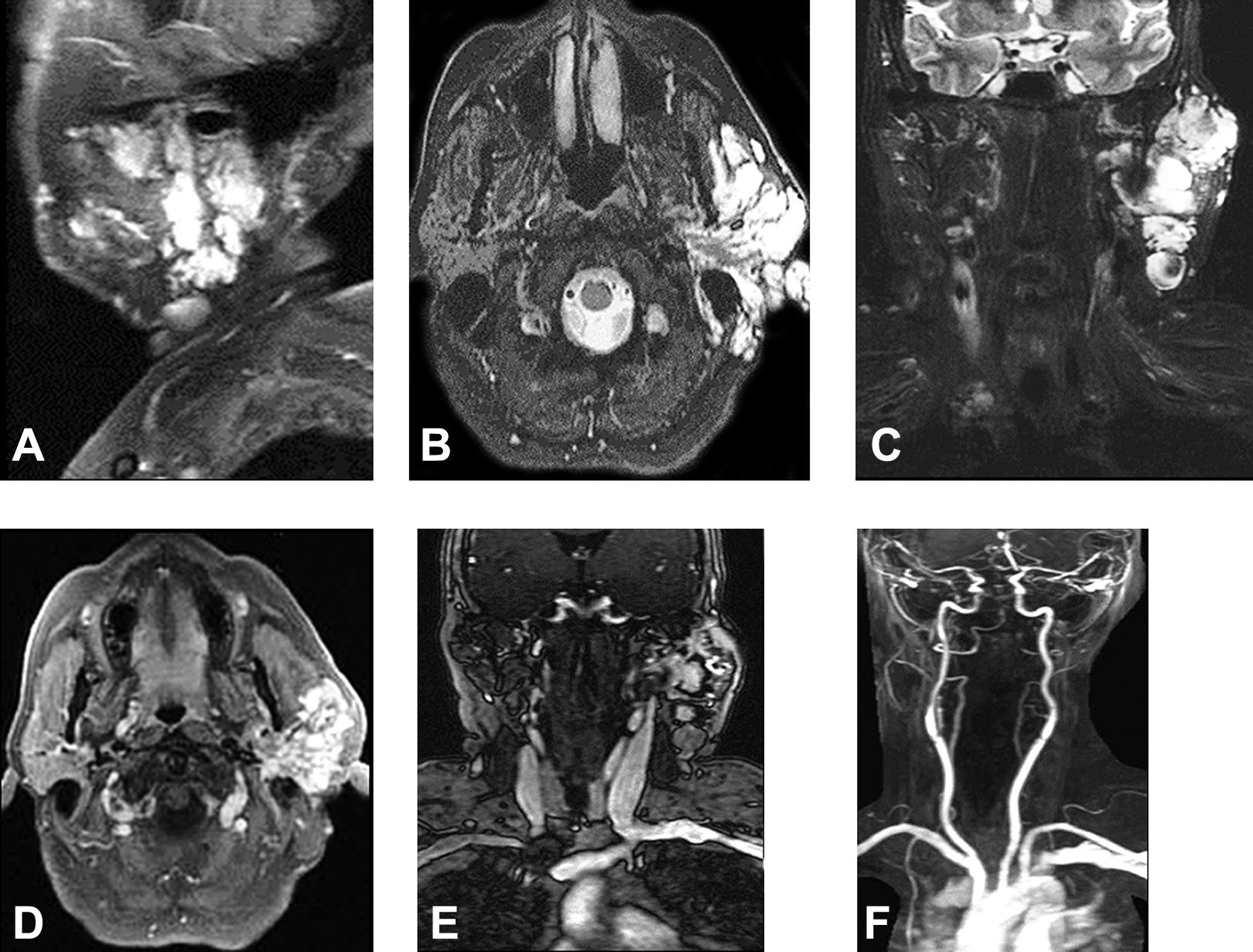
Magnetic resonance (MR) examination. T2-weighted images in sagittal (A), axial (B), and coronal (C) planes respectively reveal a lobulated hyperintense mass in the left parotid region. MR axial T1-weighted postcontrast (D) demonstrates marked enhancement of the lobulated mass. Coronal MR venogram (E) reveals dilated venous structures within the mass while coronal MR arteriogram (F) does not demonstrate arterial blood flow. Imaging findings are consistent with a left parotid venous malformation.
Discussion
Venous malformations are congenital, low-flow vascular lesions comprised of abnormally dilated veins within an ectatic venous network. 1 –3 According to the International Society for Study of Vascular Anomalies classification system, VMs can be subdivided into 6 distinct groups: common VMs, familial VMs, cutaneomucosal VMs, Blue rubber bleb nevus (Bean) syndrome VMs, glomuvenous malformations, and cerebral cavernous malformations. 4 This entity is the result of congenital, localized defects of vascular morphogenesis that occur between the 4th and 10th week of intrauterine life. 5,6 Venous malformations tend to growth steadily in proportion to somatic growth during childhood and progressively continue to increase in size throughout a patient’s life. 4,5 Although VMs are the second most common vascular lesions of the head and neck after hemangiomas, they are very rarely seen in the parotid region. 5,7,8 Vascular malformations such as VMs account for only 1.6% of all parotid tumefactions. 8
Clinical manifestation of VMs include cutaneous purplish discoloration, hyperthermia over the lesion, subjective feelings of regional pulsations, pulsatile tinnitus, dysphonia, facial paralysis secondary to facial nerve compression, among others. 2,3,5
Computed tomography is typically the preferred imaging modality employed in the evaluation of a neck mass; however, MR imaging is considered complementary. 9 Both CT and MR images are performed with the use of intravenous contrast, and adjunct angiographic and venographic sequences may provide additional information about lesion vascularity. 9 On MR imaging, VMs typically demonstrate T2-weighted signal hyperintensity and intermediate T1-weighted signal. 1,3 Perilesional T2 hyperintensity may be present due to edema and venous congestion. 1,3 Postcontrast MR images classically demonstrate enlarged, tubular vascular channels that may or may not be associated with a soft tissue mass. 1,5,8 Since VMs are low-flow lesions, MR images should lack signal flow voids, while MR angiography and venography should demonstrate absent arterial and abundant venous flow, respectively. 1,3
Differential diagnosis for a vascular mass of the parotid gland comprise arteriovenous, venous and venolymphatic malformations, hemangiomas, and a large range of tumors such as cyst adenolymphoma and pleomorphic adenoma, among others. 8
Treatment options for parotid VMs include observation, elevation, compression, laser therapy, sclerotherapy, and surgical excision. 2,5,6 Conservative measures such as lesion elevation and warm compress treatment are generally reserved for small, asymptomatic cases. 5,6 Laser therapy is considered the mainstay of management for cutaneomucosal VMs. 5,6 For parotid VMs, sclerotherapy is highlighted as a safe and effective treatment. 3,5,6 Surgical excision may be an effective treatment option for VMs that do not respond adequately to sclerotherapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.