
Abstract
Turbinate pneumatization (TP) is the most commonly observed anatomical variation of the lateral nasal wall. Although it is frequently seen in the middle turbinate, it is less frequently seen in the superior turbinate. Inferior TP is rarely seen and there are few cases reported in the literature. 1 There are 4 cases with pneumatization of all turbinates in the literature. 2 –5
Imaging Clinic
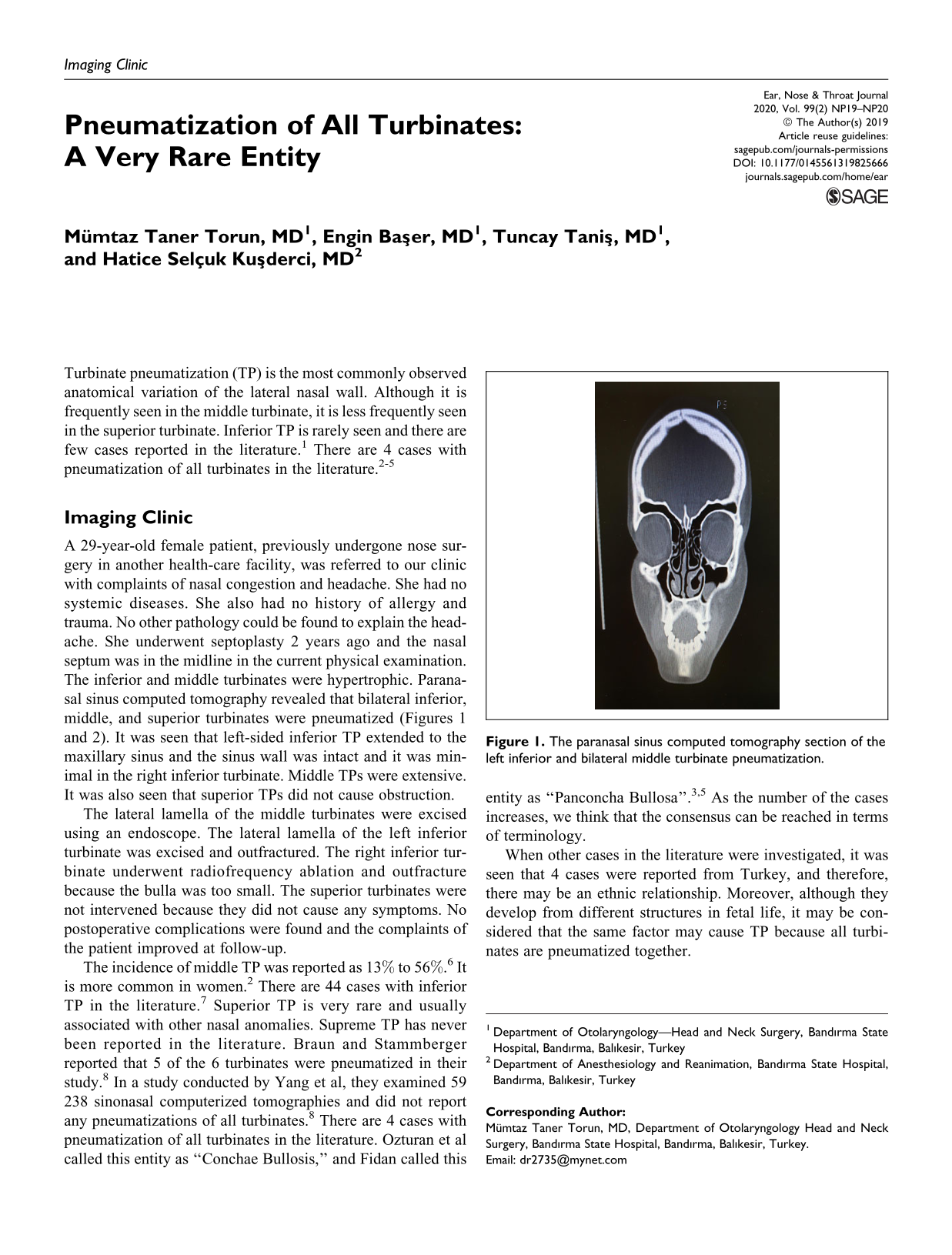
A 29-year-old female patient, previously undergone nose surgery in another health-care facility, was referred to our clinic with complaints of nasal congestion and headache. She had no systemic diseases. She also had no history of allergy and trauma. No other pathology could be found to explain the headache. She underwent septoplasty 2 years ago and the nasal septum was in the midline in the current physical examination. The inferior and middle turbinates were hypertrophic. Paranasal sinus computed tomography revealed that bilateral inferior, middle, and superior turbinates were pneumatized (Figures 1 and 2). It was seen that left-sided inferior TP extended to the maxillary sinus and the sinus wall was intact and it was minimal in the right inferior turbinate. Middle TPs were extensive. It was also seen that superior TPs did not cause obstruction.

The paranasal sinus computed tomography section of the left inferior and bilateral middle turbinate pneumatization.

The paranasal sinus computed tomography section of the right inferior, bilateral middle, and bilateral superior turbinate pneumatization.
The lateral lamella of the middle turbinates were excised using an endoscope. The lateral lamella of the left inferior turbinate was excised and outfractured. The right inferior turbinate underwent radiofrequency ablation and outfracture because the bulla was too small. The superior turbinates were not intervened because they did not cause any symptoms. No postoperative complications were found and the complaints of the patient improved at follow-up.
The incidence of middle TP was reported as 13% to 56%. 6 It is more common in women. 2 There are 44 cases with inferior TP in the literature. 7 Superior TP is very rare and usually associated with other nasal anomalies. Supreme TP has never been reported in the literature. Braun and Stammberger reported that 5 of the 6 turbinates were pneumatized in their study. 8 In a study conducted by Yang et al, they examined 59 238 sinonasal computerized tomographies and did not report any pneumatizations of all turbinates. 8 There are 4 cases with pneumatization of all turbinates in the literature. Ozturan et al called this entity as “Conchae Bullosis,” and Fidan called this entity as “Panconcha Bullosa”. 3,5 As the number of the cases increases, we think that the consensus can be reached in terms of terminology.
When other cases in the literature were investigated, it was seen that 4 cases were reported from Turkey, and therefore, there may be an ethnic relationship. Moreover, although they develop from different structures in fetal life, it may be considered that the same factor may cause TP because all turbinates are pneumatized together.
Turbinate pneumatizations can cause symptoms such as nasal obstruction, headache, nose bleeding, smelling disorders, and postnasal drainage. In addition, it can create a predisposition for sinusitis by disrupting the mucociliary clearance and reducing sinus ventilation. Sometimes it is found incidentally during radiological examinations. The computed tomography reveals precisely TP.
Turbinate pneumatizations do not require treatment if they are asymptomatic. When symptoms occur, the treatment is surgery. The most commonly used techniques are outfracture, crushing, partial excision, turbinoplasty, radiofrequency ablation, and microdebrider surgery. Crushing and partial resection techniques are preferred for the middle turbinate. The excision of the lateral lamella of the turbinate is the most commonly used method. Because there are a few cases of the inferior TP in the literature, there is no consensus on the method to be used in the treatment. When the studies in the literature were examined, it was found that crushing, outfracture, and soft tissue ablation methods were used together. 2 –4 If there is a mucosal pathology, radiofrequency ablation can be combined. Turbinoplasty is contraindicated if inferior TP is associated with the maxillary sinus because it may result in the formation of a second ostium. 2 In addition, total turbinectomy is not performed because it may cause atrophic rhinitis. Superior TP is mostly asymptomatic, and also crushing and outfracture can be performed if necessary. 2
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.