
Abstract
A young female patient presented to ear, nose, and throat clinic with long history of left sided facial pain exacerbated while flying and being in high altitude. Examination of nasal cavity and computed tomography scan of sinuses suggested left maxillary sinus barotrauma. Endoscopic sinus surgery was performed completely resolving her symptoms. Based on her symptoms and examination findings she had reverse squeeze sinus barotrauma.
A 27-year-old female presented to ear, nose, and throat (ENT) clinic with intermittent excruciating stabbing-like left-sided facial pain with associated numbness in the left upper lip area and nasal and facial congestion, left-sided rhinorhoea, and eye watering lasting for days with weeks of symptom-free periods. For 3 years, she was investigated and treated by neurologists for suspected trigeminal autonomic cephalgia manifesting as atypical facial pain and maxillofacial doctors for a dental cause.
The patient had tried nasal steroid sprays and oral antihistamines with no improvement. On direct questioning, the symptoms were exacerbated while flying, especially during ascent, and while being in high altitude on mountains above 2000 m.
Nasal endoscopy of left nasal cavity revealed mild bulge of uncinate process without polyps or mucopus. Computed tomography (CT) scan of sinuses showed large left maxillary sinus with bulging of uncinate narrowing the left side nasal cavity with no mucosal disease (Figure 1) suggesting left maxillary sinus barotrauma. Magnetic resonance imaging scan of head, performed 3 years ago, shows symmetric maxillary sinuses (Figure 2) with no other abnormalities suggesting gradual increase in size of left maxillary sinus.
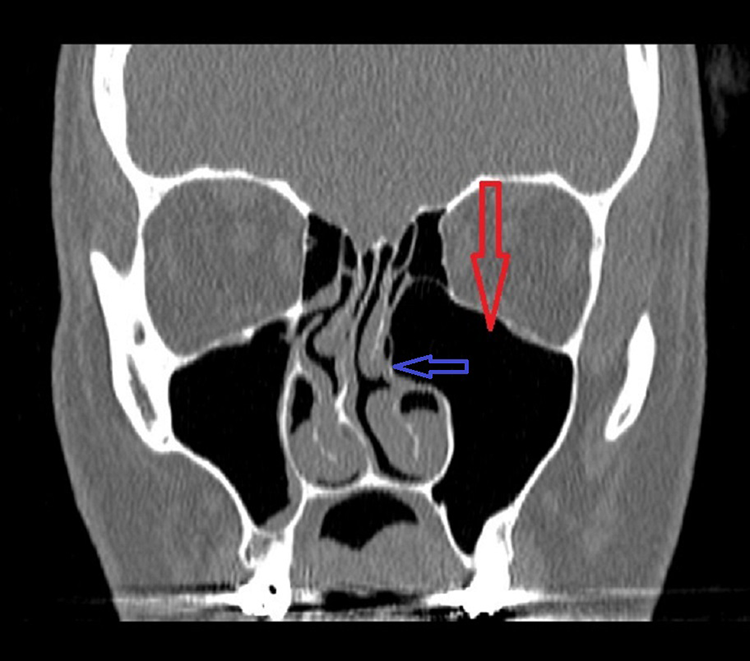
Computed tomography scan of sinuses. Large left maxillary sinus (red arrow) with bulging of uncinate process (blue arrow).
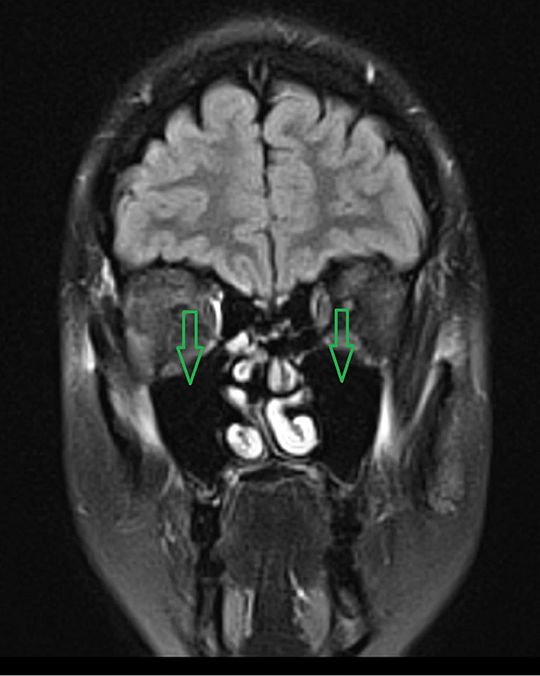
Magnetic resonance imaging scan of head. Symmetrical size of maxillary sinuses (green arrows).
Endoscopic sinus surgery was performed for left-sided uncinectomy and creating large middle meatal antrostomy. Mucosa of maxillary sinus looked healthy. Six weeks following the surgery, she was reviewed in ENT clinic with her symptoms completely resolved.
Sinus barotrauma or aerosinusitis is caused by inability to equilibrate the pressure in the sinuses caused by a rapid change in barometric pressure difference between the intrasinusal air and the surrounding atmosphere. 1 -3 It is 4 to 6 times less common than middle ear barotrauma. 4 Since the sinuses are not equipped with an active pressure equalization system like the Eustachian tube, rhinologic pressure differences cannot be controlled and can cause devastating sequelae. 4,5
The frontal sinus is affected in 70% to 80%, the maxillary sinus in 19% to 29%, less frequently ethmoidal or sphenoid sinuses. 2 -5 The pain is unilateral in more than 85%. 3,5
Sudden sharp facial pain or headache is the most common symptom, localizing to the frontal areas, less commonly to the temporal, occipital, or retrobulbar region. 1,2,4 Epistaxis or serosanguinous secretions from the nose may occur. Neurological symptoms may affect the adjacent fifth cranial nerve. 1,2
Sinus barotrauma is classified into 2 groups: squeeze and reverse squeeze. Squeeze is produced on descent when trapped air in the sinuses contracts and produces negative pressure causing mucosal edema, transudation, and mucosal or submucosal hematoma. If the outlet is blocked during ascent, reverse squeeze appears. Squeeze is more common by a ratio of at least 2:1, while reverse squeeze has more severe sequelae. 3,4 Based on worse pain during ascent and significantly bigger left maxillary sinus on CT sinus scan, our patient had reverse squeeze barotrauma.
Reverse squeeze generally results from intrasinus pathology. The air that escapes the sinus by nonphysiologic routes during a reverse squeeze can cause subcutaneous or orbital emphysema, blindness, pneumocephalus, meningitis, and trigeminal nerve dysfunction. 4 Our patient had paraesthesia of left side of upper lip innervated by trigeminal nerve and no intrasinus pathology was found radiologically and intraoperatively.
Treatment is aimed at reestablishing sinus ventilation and decreasing mucosal inflammation with analgesics and intranasal and oral decongestants, a tapering course of steroids. 1,2,4 Endoscopic sinus surgery may be required to enlarge the natural ostium to regain appropriate sinus ventilation as it was in our patient’s case. 1,2
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.